

Blunted tachycardia and cardiac sympathetic denervation in isolated rapid eye movement sleep behavior disorder
- PMID: 39232705
- PMCID: PMC11373284
- DOI: 10.1186/s12883-024-03822-w
Blunted tachycardia and cardiac sympathetic denervation in isolated rapid eye movement sleep behavior disorder
Abstract
Background: Isolated rapid eye movement sleep behavior disorder (iRBD) serves as a prodromal phase of Parkinson's disease (PD) and dementia with Lewy bodies (DLB). Blunted tachycardia (BT) during postural changes indicates neurogenic orthostatic hypotension, a marker of autonomic dysfunction. We aimed to investigate whether BT is associated with cardiac sympathetic neurogenic denervation. Additionally, we conducted a preliminary short-term follow-up to examine the potential prognostic significance of BT regarding phenoconversion and mortality.
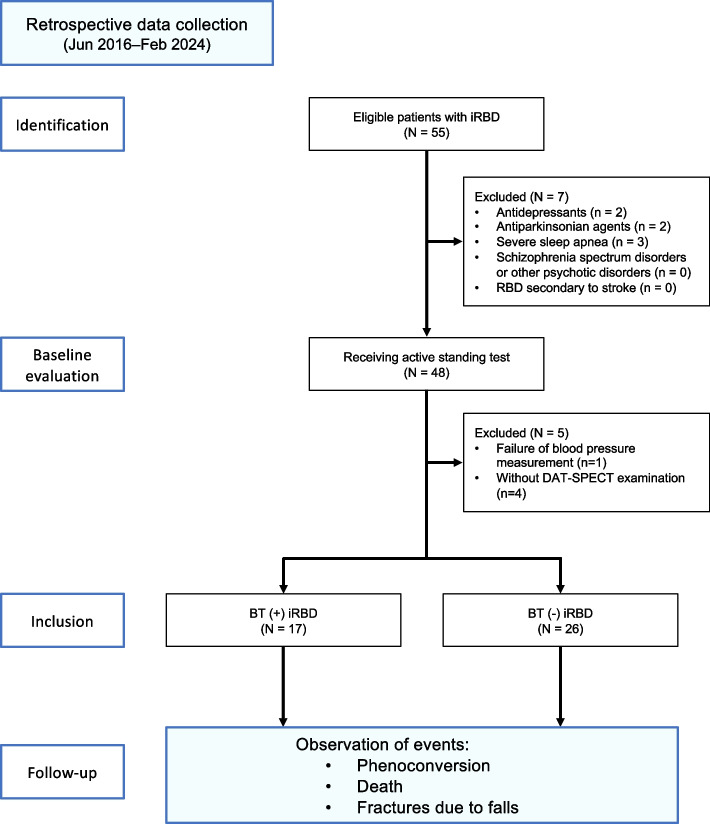
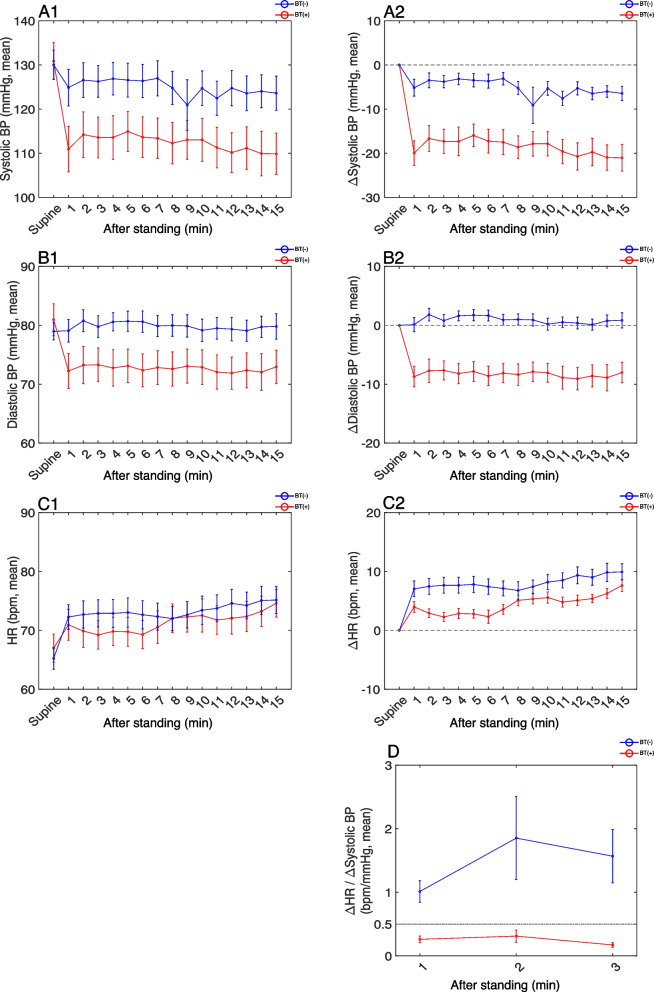
Methods: Forty-three patients with iRBD at Shiga University of Medical Science Hospital underwent active standing tests to identify BT, defined by a specific ratio of decrease in systolic blood pressure to inadequate increase in heart rate after standing, and orthostatic hypotension. 123I-metaiodobenzylguanidine myocardial scintigraphy (123I-MIBG) and dopamine transporter single-photon emission computed tomography (DAT-SPECT) were performed. Participants were followed up for 3.4 ± 2.4 years for phenoconversion and 4.0 ± 2.3 years for mortality assessment, and the risk of events was analyzed using log-rank tests.
Results: Among the 43 participants (mean age, 72.3 ± 7.9 years; 8 female), 17 met the BT criteria. We found no significant comorbidity-related differences in hypertension or diabetes between the BT(+) and BT(-) groups. Orthostatic hypotension was more prevalent in the BT(+) group than in the BT(-) group (47.1% vs 7.7%, p = 0.003). BT(+) patients were older with a lower early and delayed MIBG uptake; however, no significant differences were observed in DAT accumulation. Phenoconversion was observed in seven (41.2%) BT(+) and seven (26.9%) BT(-) patients. Three deaths were recorded in the BT(+) group (17.6%) and three in the BT(-) group (11.5%). No significant differences were observed in the risk of phenoconversion or mortality between the groups.
Conclusions: We have identified the possibility that BT reflects cardiac sympathetic neurogenic denervation in patients with iRBD. Future research is needed to elucidate the potential prognostic value of BT.
Keywords: Autonomic dysfunction; Blunted tachycardia; Longitudinal study; Orthostatic hypotension; Phenoconversion; Rapid eye movement sleep behavior disorder.
© 2024. The Author(s).
Conflict of interest statement
Hiroshi Kadotani was supported by donations from Fukuda Life Tech Co., Ltd., Fukuda Life Tech Keiji Co., Ltd., and Kadotani Kids Clinic to the Shiga University of Medical Science. Hiroshi Kadotani received Merck Sharp and Dohme Corp/MSD K.K. (the Investigator-initiated Studies Program), Eisai Co., Ltd., and the SECOM Science and Technology Foundation. The opinions expressed in this paper are those of the authors and do not necessarily represent those of Merck Sharp and Dohme Corp/MSD K.K. The other authors declare no conflicts of interest.
Figures
References
-
- American Academy of Sleep Medicine. International classification of sleep disorders. 3rd ed. Darien. American Academy of Sleep Medicine; 2014.
-
- Boeve BF. REM sleep behavior disorder: Updated review of the core features, the REM sleep behavior disorder-neurodegenerative disease association, evolving concepts, controversies, and future directions. Ann N Y Acad Sci. 2010;1184:15–54. 10.1111/j.1749-6632.2009.05115.x. 10.1111/j.1749-6632.2009.05115.x - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
