

Risk of SARS-CoV-2 infection in professional settings, shops, shared transport, and leisure activities in France, 2020-2022
- PMID: 39232732
- PMCID: PMC11376041
- DOI: 10.1186/s12889-024-19651-y
Risk of SARS-CoV-2 infection in professional settings, shops, shared transport, and leisure activities in France, 2020-2022
Abstract
Purpose: The aim of the study was to identify settings associated with SARS-CoV-2 transmission throughout the COVID-19 pandemic in France.
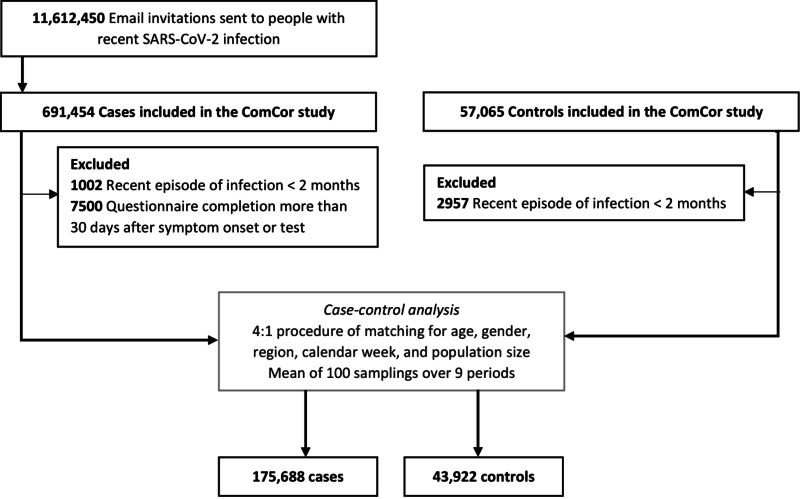
Methods: Cases with recent SARS-CoV-2 infection were matched with controls (4:1 ratio) on age, sex, region, population size, and calendar week. Odds ratios for SARS-CoV-2 infection were estimated for nine periods in models adjusting for socio-demographic characteristics, health status, COVID-19 vaccine, and past infection.
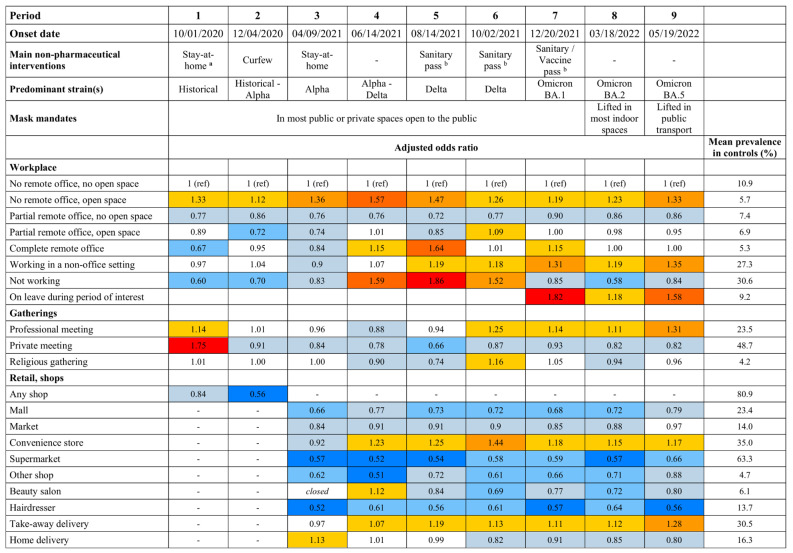
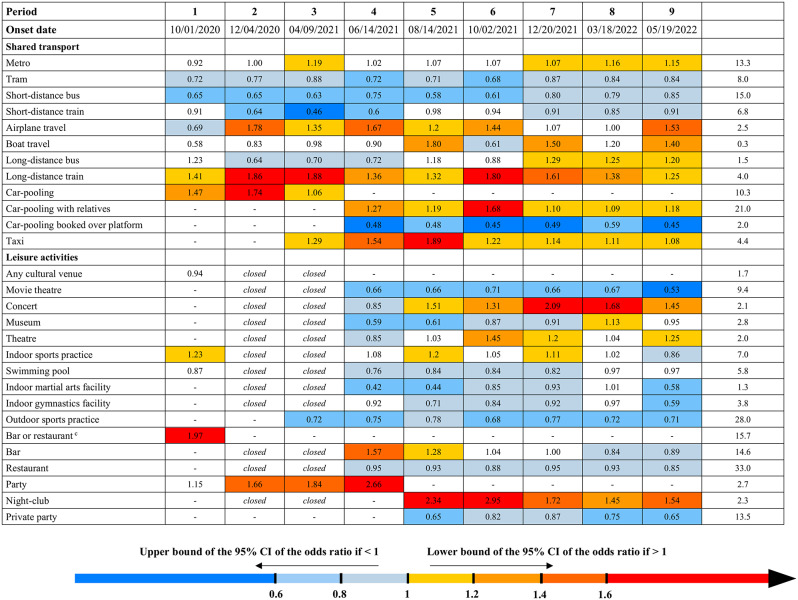
Results: Between October 27, 2020 and October 2, 2022, 175,688 cases were matched with 43,922 controls. An increased risk of infection was documented throughout the study for open-space offices compared to offices without open space (OR range across the nine periods: 1.12 to 1.57) and long-distance trains (1.25 to 1.88), and during most of the study for convenience stores (OR range in the periods with increased risk: 1.15 to 1.44), take-away delivery (1.07 to 1.28), car-pooling with relatives (1.09 to 1.68), taxis (1.08 to 1.89), airplanes (1.20 to 1.78), concerts (1.31 to 2.09) and night-clubs (1.45 to 2.95). No increase in transmission was associated with short-distance shared transport, car-pooling booked over platforms, markets, supermarkets and malls, hairdressers, museums, movie theatres, outdoor sports, and swimming pools. The increased risk of infection in bars and restaurants was no longer present in restaurants after reopening in June 2021. It persisted in bars only among those aged under 40 years.
Conclusion: Closed settings in which people are less likely to wear masks were most affected by SARS-CoV-2 transmission and should be the focus of air quality improvement.
Clinicaltrials: GOV (03/09/2022): NCT04607941.
Keywords: Case-control studies; Infectious disease transmission; Leisure activities; Occupational exposure; SARS-CoV-2; Travel; Workplace.
© 2024. The Author(s).
Conflict of interest statement
Fabrice Carrat declares consulting fee from Sanofi on influenza epidemiology. Authors declare no further interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
