

Effect of perioperative sigh ventilation on postoperative hypoxemia and pulmonary complications after on-pump cardiac surgery (E-SIGHT): study protocol for a randomized controlled trial
- PMID: 39232795
- PMCID: PMC11373100
- DOI: 10.1186/s13063-024-08416-y
Effect of perioperative sigh ventilation on postoperative hypoxemia and pulmonary complications after on-pump cardiac surgery (E-SIGHT): study protocol for a randomized controlled trial
Abstract
Background: Postoperative hypoxemia and pulmonary complications remain a frequent event after on-pump cardiac surgery and mostly characterized by pulmonary atelectasis. Surfactant dysfunction or hyposecretion happens prior to atelectasis formation, and sigh represents the strongest stimulus for surfactant secretion. The role of sigh breaths added to conventional lung protective ventilation in reducing postoperative hypoxemia and pulmonary complications among cardiac surgery is unknown.
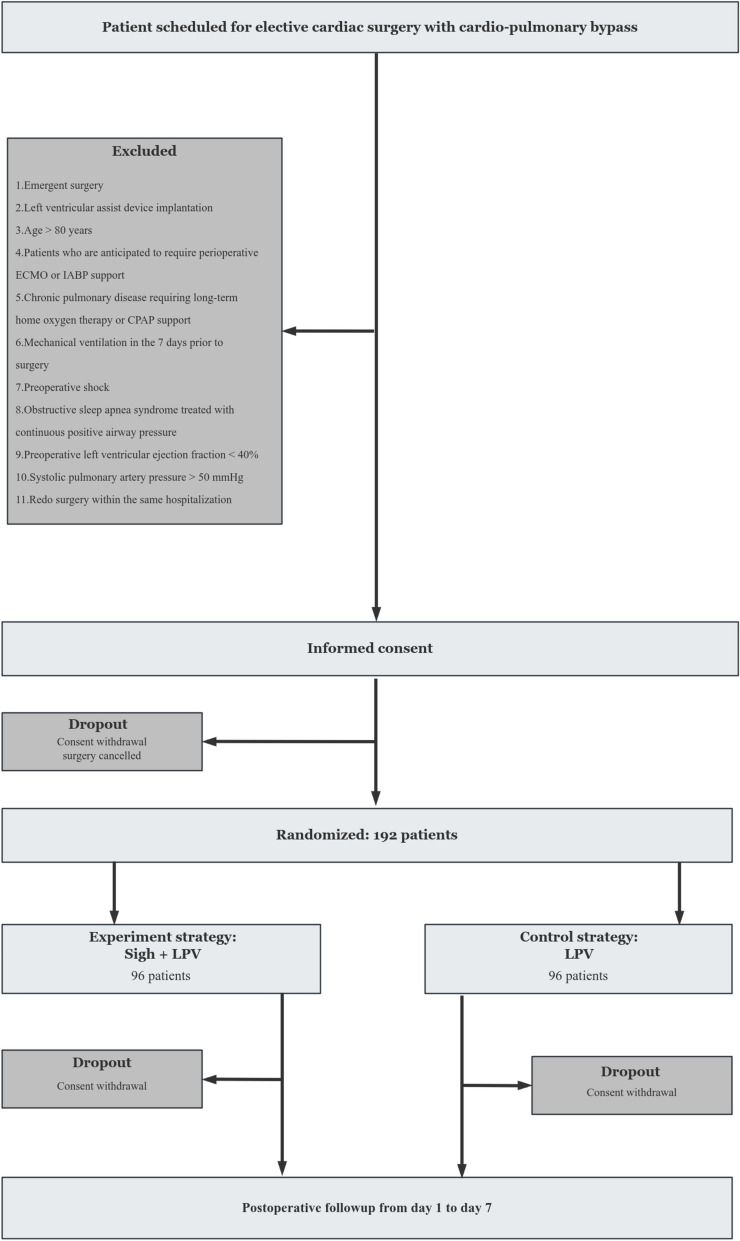
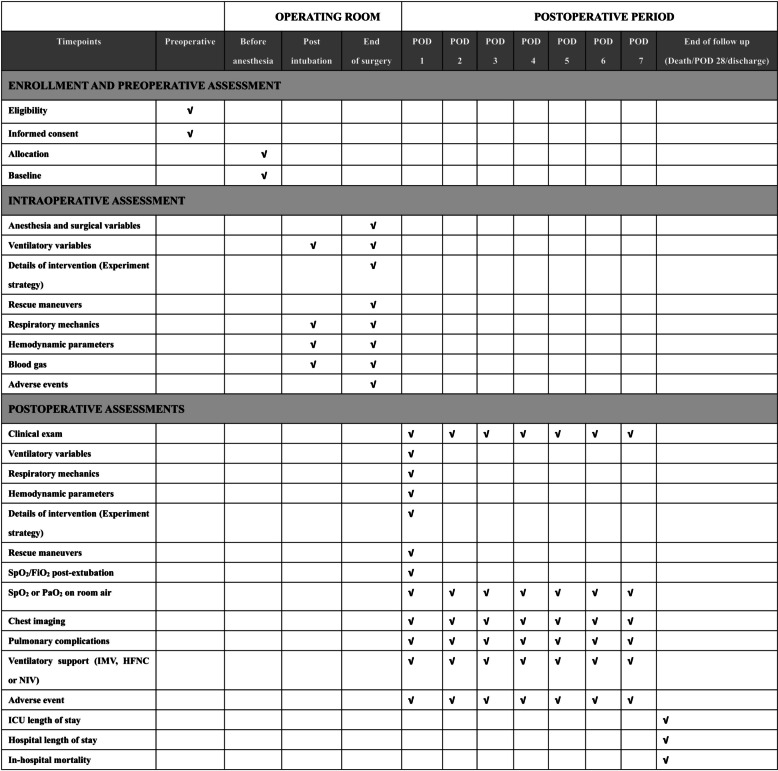
Methods: The perioperative sigh ventilation in cardiac surgery (E-SIGHT) trial is a single-center, two-arm, randomized controlled trial. In total, 192 patients scheduled for elective cardiac surgery with cardiopulmonary bypass (CPB) and aortic cross-clamp will be randomized into one of the two treatment arms. In the experimental group, besides conventional lung protective ventilation, sigh volumes producing plateau pressures of 35 cmH2O (or 40 cmH2O for patients with body mass index > 35 kg/m2) delivered once every 6 min from intubation to extubation. In the control group, conventional lung protective ventilation without preplanned recruitment maneuvers is used. Lung protective ventilation (LPV) consists of low tidal volumes (6-8 mL/kg of predicted body weight) and positive end-expiratory pressure (PEEP) setting according to low PEEP/FiO2 table for acute respiratory distress syndrome (ARDS). The primary endpoint is time-weighted average SpO2/FiO2 ratio during the initial post-extubation hour. Main secondary endpoint is the severity of postoperative pulmonary complications (PPCs) computed by postoperative day 7.
Discussion: The E-SIGHT trial will be the first randomized controlled trial to evaluate the impact of perioperative sigh ventilation on the postoperative outcomes after on-pump cardiac surgery. The trial will introduce and assess a novel perioperative ventilation approach to mitigate the risk of postoperative hypoxemia and PPCs in patients undergoing cardiac surgery. Also provide the basis for a future larger trial aiming at verifying the impact of sigh ventilation on postoperative pulmonary complications.
Trial registration: ClinicalTrials.gov NCT06248320. Registered on January 30, 2024. Last updated February 26, 2024.
Keywords: Cardiac surgery; Cardiopulmonary bypass; Mechanical ventilation; Postoperative hypoxemia; Postoperative pulmonary complications; Sigh.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
A perioperative surgeon-controlled open-lung approach versus conventional protective ventilation with low positive end-expiratory pressure in cardiac surgery with cardiopulmonary bypass (PROVECS): study protocol for a randomized controlled trial.Trials. 2018 Nov 13;19(1):624. doi: 10.1186/s13063-018-2967-y. Trials. 2018. PMID: 30424770 Free PMC article.
-
Individualized flow-controlled versus conventional pressure-controlled ventilation in on-pump heart surgery (FLOWVENTIN HEARTSURG): study protocol for a randomized controlled trial.Trials. 2023 Mar 16;24(1):195. doi: 10.1186/s13063-023-07201-7. Trials. 2023. PMID: 36922825 Free PMC article.
-
Effects of intraoperative individualized PEEP on postoperative atelectasis in obese patients: study protocol for a prospective randomized controlled trial.Trials. 2020 Jul 6;21(1):618. doi: 10.1186/s13063-020-04565-y. Trials. 2020. PMID: 32631414 Free PMC article.
-
Perioperative ventilatory strategies in cardiac surgery.Best Pract Res Clin Anaesthesiol. 2015 Sep;29(3):381-95. doi: 10.1016/j.bpa.2015.08.006. Epub 2015 Sep 4. Best Pract Res Clin Anaesthesiol. 2015. PMID: 26643102 Free PMC article. Review.
-
Recruitment maneuvers to reduce pulmonary atelectasis after cardiac surgery: A meta-analysis of randomized trials.J Thorac Cardiovasc Surg. 2022 Jul;164(1):171-181.e4. doi: 10.1016/j.jtcvs.2020.10.142. Epub 2020 Nov 26. J Thorac Cardiovasc Surg. 2022. PMID: 33341273 Review.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
