

Comparison of Different Head Tilt Angles in Tomotherapy and Volumetric Modulated Arc Therapy for Hippocampal-Avoidance Whole-Brain Radiotherapy
- PMID: 39233627
- PMCID: PMC11375751
- DOI: 10.1177/15330338241281326
Comparison of Different Head Tilt Angles in Tomotherapy and Volumetric Modulated Arc Therapy for Hippocampal-Avoidance Whole-Brain Radiotherapy
Abstract
Purpose: Hippocampal-avoidance whole-brain radiotherapy (HA-WBRT) planning can present challenges. This study examines the influence of head tilt angles on the dosimetric characteristics of target and organs at risk (OARs), aiming to identify the optimal tilt angle that yields optimal dosimetric outcomes using tomotherapy (TOMO).
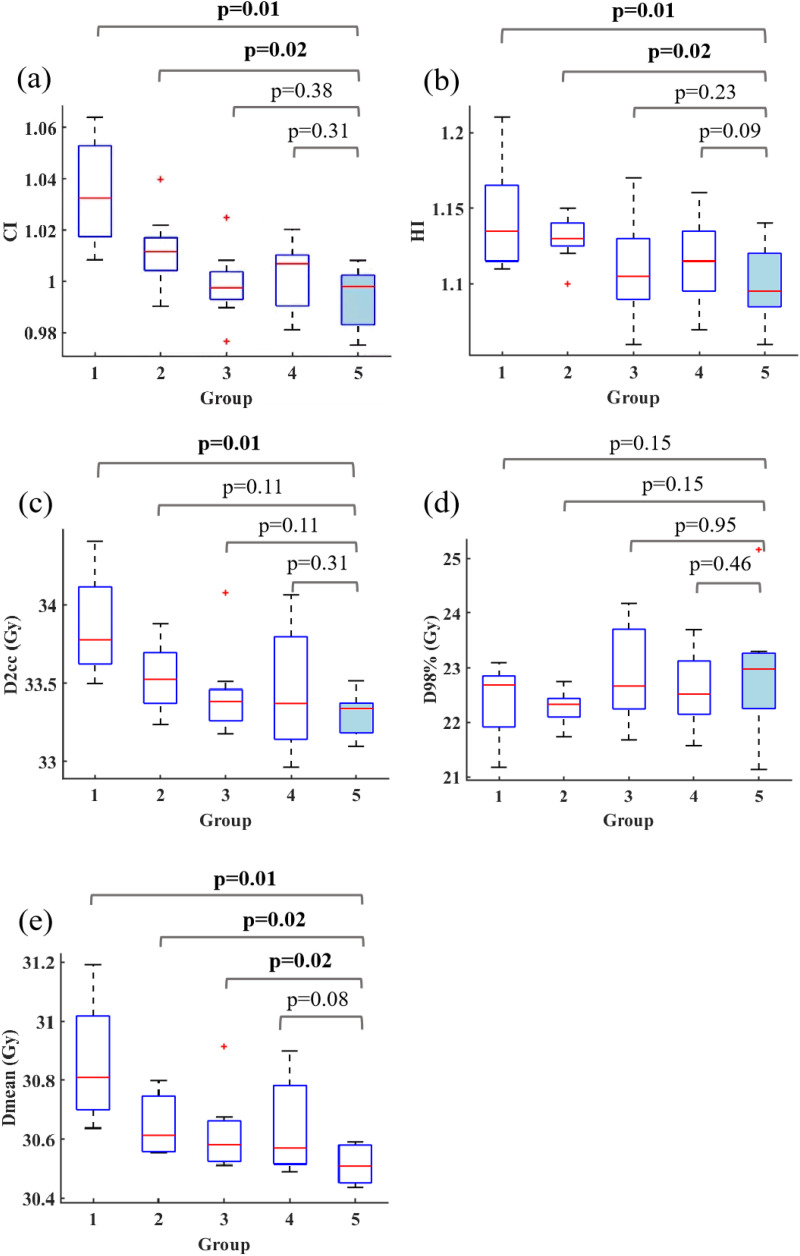
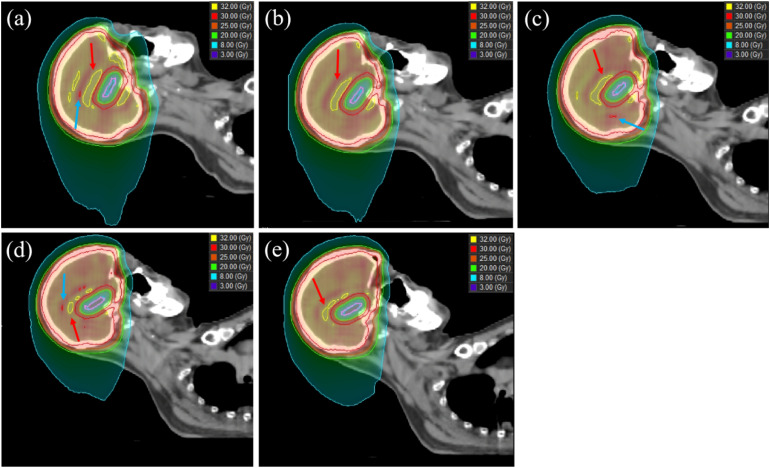
Methods: Eight patients diagnosed with brain metastases underwent CT scans at five tilt angles: [0°, 10°), [10°, 20°), [20°, 30°), [30°, 40°), and [40°, 45°]. Treatment plans were generated using TOMO and volumetric modulated arc therapy (VMAT). Dosimetric parameters including conformity index (CI), homogeneity index (HI), D2cc, D98%, and Dmean of PTV, as well as Dmax, and Dmean of OARs were analyzed. Furthermore, a comparison was made between the dosimetric parameters of TOMO and VMAT plans. Finally, delivery efficiency of TOMO plans were assessed.
Results: For the PTV, [40°, 45°] tilt angle demonstrated significantly better conformity, homogeneity, lower D2cc, and lower Dmean for the PTV. Regarding the OARs, the [40°, 45°] head tilt angle demonstrated significantly lower Dmax and Dmean in hippocampus, eyes, optic chiasm, and optic nerves. The [40°, 45°] tilt angle also showed significantly lower Dmax for brainstem and cochleas, as well as a lower Dmean for lens. In the [40°,45°] tilt angle for HA-WBRT, TOMO showed superior performance over VMAT for the PTV. TOMO achieved lower Dmax for brainstem, cochleas, optic nerves, and optic chiasm, as well as a lower Dmean for hippocampus. Furthermore, a significant correlation was found between delivery time and the PTV projection length in the sagittal plane.
Conclusion: The TOMO plan utilizing a tilt angle range of [40°, 45°] demonstrated superior PTV conformity and uniformity, along with enhanced OARs sparing. Furthermore, it exhibited a dosimetric advantage over VMAT for PTV and most OARs at the same angle range.
Keywords: dosimetry; efficacy; hippocampus; radiotherapy; tomotherapy.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




Similar articles
-
Dosimetric comparison of HyperArc, conventional noncoplanar VMAT, and Halcyon-based coplanar VMAT in hippocampal-sparing whole-brain radiotherapy.Med Dosim. 2025 Autumn;50(3):216-221. doi: 10.1016/j.meddos.2025.01.007. Epub 2025 Feb 20. Med Dosim. 2025. PMID: 39984398
-
Dosimetric effect of collimator rotation on intensity modulated radiotherapy and volumetric modulated arc therapy for rectal cancer radiotherapy.J Xray Sci Technol. 2024;32(5):1331-1348. doi: 10.3233/XST-240172. J Xray Sci Technol. 2024. PMID: 39093110
-
Dosimetric evaluation of a novel automated noncoplanar volumetric modulated arc therapy technique for treating optic nerve sheath meningiomas.Front Oncol. 2025 Jun 27;15:1531918. doi: 10.3389/fonc.2025.1531918. eCollection 2025. Front Oncol. 2025. PMID: 40657256 Free PMC article.
-
Helical tomotherapy for whole-brain irradiation with integrated boost to multiple brain metastases: evaluation of dose distribution characteristics and comparison with alternative techniques.Int J Radiat Oncol Biol Phys. 2013 Jul 15;86(4):734-42. doi: 10.1016/j.ijrobp.2013.03.031. Epub 2013 May 14. Int J Radiat Oncol Biol Phys. 2013. PMID: 23680034 Clinical Trial.
-
Dosimetric comparison between Intensity Modulated Radiation Therapy (IMRT) vs dual arc Volumetric Arc Therapy (VMAT) for nasopharyngeal cancer (NPC): Systematic review and meta-analysis.J Med Imaging Radiat Sci. 2023 Mar;54(1):167-177. doi: 10.1016/j.jmir.2022.10.195. Epub 2022 Nov 29. J Med Imaging Radiat Sci. 2023. PMID: 36456460
References
-
- Mehta MP, Khuntia DJN. Current strategies in whole-brain radiation therapy for brain metastases. Neurosurgery. 2005;57(5):S4-33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
