Boundary-based registration improves sensitivity for detecting hypoperfusion in sporadic frontotemporal lobar degeneration
- PMID: 39233675
- PMCID: PMC11371585
- DOI: 10.3389/fneur.2024.1452944
Boundary-based registration improves sensitivity for detecting hypoperfusion in sporadic frontotemporal lobar degeneration
Abstract
Introduction: Frontotemporal lobar degeneration (FTLD) is associated with FTLD due to tau (FTLD-tau) or TDP (FTLD-TDP) inclusions found at autopsy. Arterial Spin Labeling (ASL) MRI is often acquired in the same session as a structural T1-weighted image (T1w), enabling detection of regional changes in cerebral blood flow (CBF). We hypothesize that ASL-T1w registration with more degrees of freedom using boundary-based registration (BBR) will better align ASL and T1w images and show increased sensitivity to regional hypoperfusion differences compared to manual registration in patient participants. We hypothesize that hypoperfusion will be associated with a clinical measure of disease severity, the FTLD-modified clinical dementia rating scale sum-of-boxes (FTLD-CDR).
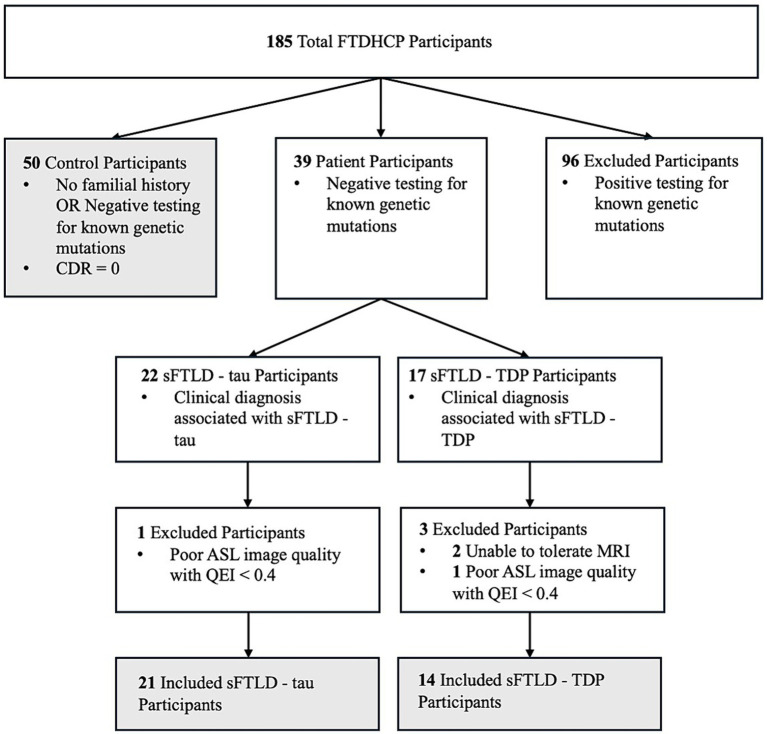
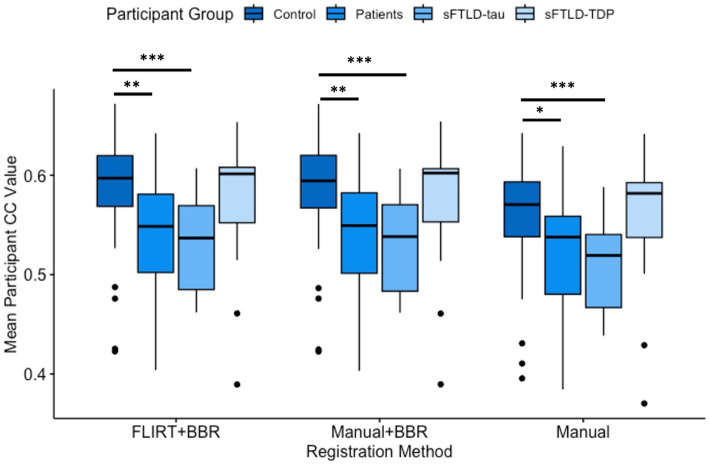
Materials and methods: Patients with sporadic likely FTLD-tau (sFTLD-tau; N = 21), with sporadic likely FTLD-TDP (sFTLD-TDP; N = 14), and controls (N = 50) were recruited from the Connectomic Imaging in Familial and Sporadic Frontotemporal Degeneration project (FTDHCP). Pearson's Correlation Coefficients (CC) were calculated on cortical vertex-wise CBF between each participant for each of 3 registration methods: (1) manual registration, (2) BBR initialized with manual registration (manual+BBR), (3) and BBR initialized using FLIRT (FLIRT+BBR). Mean CBF was calculated in the same regions of interest (ROIs) for each registration method after image alignment. Paired t-tests of CC values for each registration method were performed to compare alignment. Mean CBF in each ROI was compared between groups using t-tests. Differences were considered significant at p < 0.05 (Bonferroni-corrected). We performed linear regression to relate FTLD-CDR to mean CBF in patients with sFTLD-tau and sFTLD-TDP, separately (p < 0.05, uncorrected).
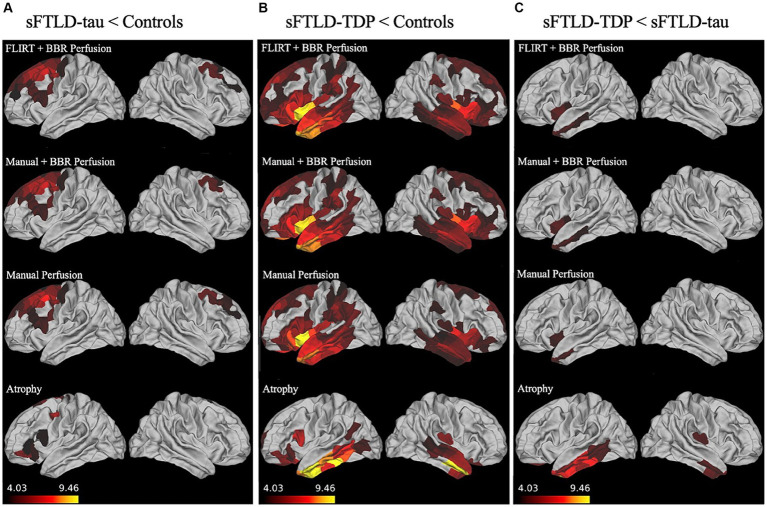
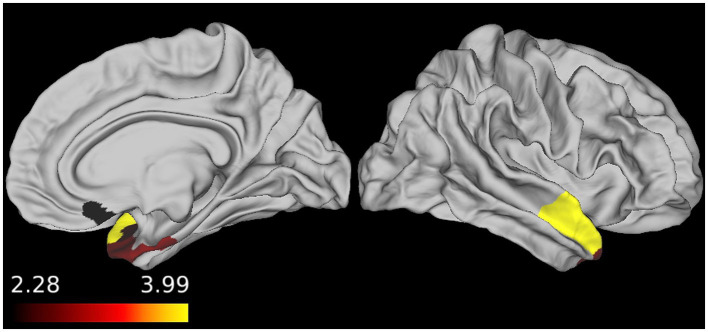
Results: All registration methods demonstrated significant hypoperfusion in frontal and temporal regions in each patient group relative to controls. All registration methods detected hypoperfusion in the left insular cortex, middle temporal gyrus, and temporal pole in sFTLD-TDP relative to sFTLD-tau. FTLD-CDR had an inverse association with CBF in right temporal and orbitofrontal ROIs in sFTLD-TDP. Manual+BBR performed similarly to FLIRT+BBR.
Discussion: ASL is sensitive to distinct regions of hypoperfusion in patient participants relative to controls, and in patients with sFTLD-TDP relative to sFTLD-tau, and decreasing perfusion is associated with increasing disease severity, at least in sFTLD-TDP. BBR can register ASL-T1w images adequately for controls and patients.
Keywords: arterial spin labeling; boundary-based registration; cerebral blood flow; frontotemporal lobar degeneration; image registration.
Copyright © 2024 Mihailescu, Hlava, Cook, Mandelli, Lee, Boeve, Dickerson, Gorno-Tempini, Rogalski, Grossman, Gee, McMillan and Olm.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures