

Caplacizumab as an add-on therapy in a 7-year-old girl with exacerbated immune-mediated thrombotic thrombocytopenic purpura, a case report and literature review
- PMID: 39233868
- PMCID: PMC11371688
- DOI: 10.3389/fped.2024.1448801
Caplacizumab as an add-on therapy in a 7-year-old girl with exacerbated immune-mediated thrombotic thrombocytopenic purpura, a case report and literature review
Abstract
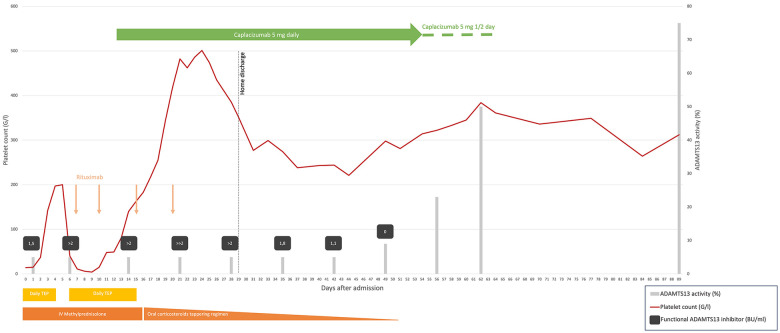
The cornerstone treatment for immune-mediated thrombotic thrombocytopenic purpura (iTTP) in children is a combination of therapeutic plasma exchange (TPE), corticosteroids, and rituximab. Caplacizumab is an anti-von Willebrand factor (VWF) NANOBODY molecule approved as a frontline therapy of iTTP for adults and children aged ≥12 years. Using caplacizumab in children aged <12 years remains a gray area based on recommendations but with no marketing authorization. We report the first case of a pediatric patient with iTTP successfully treated with a caplacizumab dose adjustment of 5 mg daily based on ADAMTS13 activity. We also review all published cases of iTTP in children aged <12 years treated with caplacizumab. This is a 7-year-old girl with clinical thrombotic microangiopathy, in the absence of diarrhea and kidney injury. With a French score of 2 and a PLASMIC score of 7 (high risk), the diagnosis of TTP was suspected and later confirmed by severely low ADAMTS13 activity (<5%). Immune-mediated TTP was distinguished from the congenital one due to the presence of a functional ADAMTS13 inhibitor. Daily TPE and intravenous corticosteroids were started on day 0 (D0). Rituximab was added on D4, and due to refractoriness under daily TPE, we considered off-label administration of caplacizumab from D12. A clinical answer, with a significant increase in the platelet count, was observed within 48 h. A complete ADAMTS13 recovery was reached on D62. No major adverse events were observed during the treatment. She was discharged from the hospital over 3 months ago with a platelet count still within normal ranges. In the literature, we identified a total of four case reports describing five iTTP patients aged <12 years treated with caplacizumab, with a 100% success and tolerability rate. These published data attest to the efficacy and safety of the systematic use of caplacizumab and rituximab as frontline therapy in pediatric iTTP under 12 years of age. Therefore, prospective data are needed to support commercial authorization of caplacizumab in this subpopulation. Close monitoring of ADAMTS13 activity is particularly of interest among children to limit the number of caplacizumab injections.
Keywords: benign hematological disorders; caplacizumab; iTTP; immune-mediated thrombotic thrombocytopenic purpura; pediatrics.
© 2024 Chavaz, Cimasoni, Kremer Hovinga, Coppo and Ansari.
Conflict of interest statement
Caplacizumab treatment was financed by Sanofi. JK is a member of the advisory board of Takeda, a member of the Takeda group of companies, for the development of recombinant ADAMTS13, and of Ablynx, now part of Sanofi for the development of caplacizumab, and has received lecture fees from Takeda and Sanofi. All honoraria are paid to her employer, Insel Gruppe AG, Bern, Switzerland. PC is a member of Sanofi's advisory board and has received honoraria for participating in symposia. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous