

Associations of Rest-Activity Rhythm Disturbances With Stroke Risk and Poststroke Adverse Outcomes
- PMID: 39234806
- PMCID: PMC11935632
- DOI: 10.1161/JAHA.123.032086
Associations of Rest-Activity Rhythm Disturbances With Stroke Risk and Poststroke Adverse Outcomes
Abstract
Background: Many disease processes are influenced by circadian clocks and display ~24-hour rhythms. Whether disruptions to these rhythms increase stroke risk is unclear. We evaluated the association between 24-hour rest-activity rhythms, stroke risk, and major poststroke adverse outcomes.
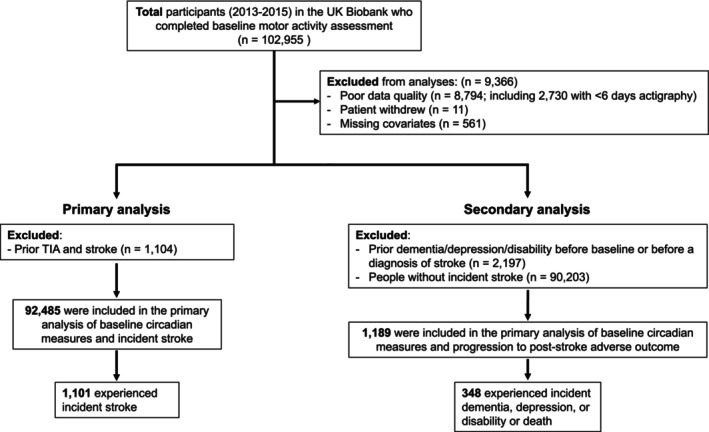
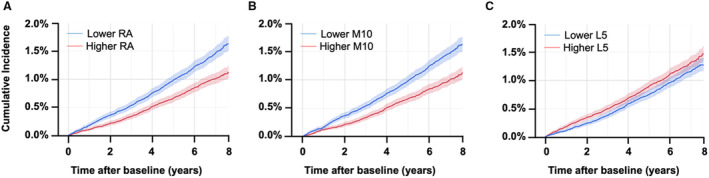
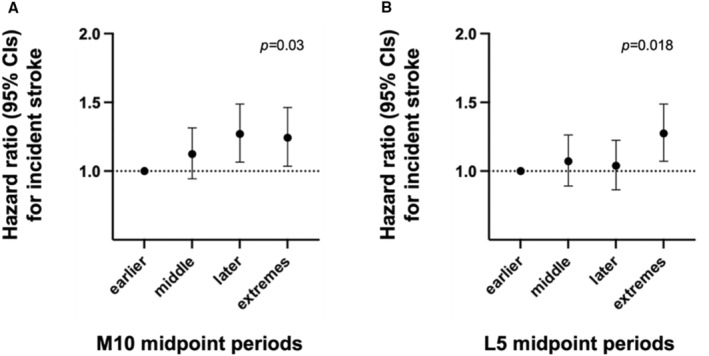
Methods and results: We examined ~100 000 participants from the UK Biobank (aged 44-79 years; ~57% women) assessed with actigraphy (6-7 days) and 5-year median follow-up. We derived (1) most active 10-hour activity counts across the 24-hour cycle and the timing of its midpoint timing; (2) the least active 5-hour count and its midpoint; (3) relative amplitude; (4) interdaily stability; and (5) intradaily variability, for stability and fragmentation of the rhythm. Cox proportional hazard models were constructed for time to (1) incident stroke (n=1652) and (2) poststroke adverse outcomes (dementia, depression, disability, or death). Suppressed relative amplitude (lowest quartile [quartile 1] versus the top quartile [quartile 4]) was associated with stroke risk (hazard ratio [HR], 1.61 [95% CI, 1.35-1.92]; P<0.001) after adjusting for demographics. Later most active 10-hour activity count midpoint timing (14:00-15:26; HR, 1.26 [95% CI, 1.07-1.49]; P=0.007) also had higher stroke risk than earlier (12:17-13:10) participants. A fragmented rhythm (intradaily variability) was also associated with higher stroke risk (quartile 4 versus quartile 1; HR, 1.26 [95% CI, 1.06-1.49]; P=0.008). Suppressed relative amplitude was associated with risk for poststroke adverse outcomes (quartile 1 versus quartile 4; HR, 2.02 [95% CI, 1.46-2.48]; P<0.001). All associations were independent of age, sex, race, obesity, sleep disorders, cardiovascular diseases or risks, and other comorbidity burdens.
Conclusions: Suppressed 24-hour rest-activity rhythm may be a risk factor for stroke and an early indicator of major poststroke adverse outcomes.
Keywords: actigraphy; daily activity rhythms; dementia; depression; disability; mortality; stroke.
Figures
Update of
-
Associations of rest-activity rhythm disturbances with stroke risk and post-stroke adverse outcomes.medRxiv [Preprint]. 2023 May 16:2023.05.14.23289966. doi: 10.1101/2023.05.14.23289966. medRxiv. 2023. Update in: J Am Heart Assoc. 2024 Sep 17;13(18):e032086. doi: 10.1161/JAHA.123.032086. PMID: 37292791 Free PMC article. Updated. Preprint.
References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore‐Mensah Y, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145:e153–e639. doi: 10.1161/CIR.0000000000001052 - DOI - PubMed
-
- Fens M, van Heugten CM, Beusmans GHMI, Limburg M, Haeren R, Kaemingk A, Metsemakers JFM. Not as transient: patients with transient ischaemic attack or minor stroke experience cognitive and communication problems; an exploratory study. Eur J Gen Pract. 2013;19:11–16. doi: 10.3109/13814788.2012.715147 - DOI - PubMed
-
- van Rooij FG, Plaizier NO, Vermeer SE, Góraj BM, Koudstaal PJ, Richard E, de Leeuw F‐E, Kessels RPC, van Dijk EJ. Executive function declines in the first 6 months after a transient ischemic attack or transient neurological attack. Stroke. 2017;48:3323–3328. doi: 10.1161/STROKEAHA.117.018298 - DOI - PubMed
-
- Towfighi A, Ovbiagele B, El Husseini N, Hackett ML, Jorge RE, Kissela BM, Mitchell PH, Skolarus LE, Whooley MA, Williams LS. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2017;48:e30–e43. doi: 10.1161/STR.0000000000000113 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
