

The role of prehabilitation in HNSCC patients treated with chemoradiotherapy
- PMID: 39235658
- PMCID: PMC11377665
- DOI: 10.1007/s00520-024-08834-3
The role of prehabilitation in HNSCC patients treated with chemoradiotherapy
Abstract
Background: Radiotherapy (RT) is used in head and neck squamous cell carcinoma (HNSCC) with excellent effectiveness, but it is burdened by important side effects, which may negatively impact patients' quality of life (QoL). In particular when associated with chemotherapy (CT), that has a radiosensitising effect (and its own toxicities), it is responsible for several adverse events, causing social discomfort and lower QoL, in patients who are already experiencing several tumor-related discomforts. Prehabilitation is a healthcare intervention consisting of several specialist visits prior to the start of treatment, with the aim of improving the patient's health status, resolving symptoms that interfere with treatment and impact QoL, and finally to better avoid or overcome complications. Of all cancer patients, HNSCC patients are among those who could benefit most from prehabilitation, both because of the high number of symptoms and toxicities and their difficult management. Despite this and the emerging data, prehabilitation is not often considered for the majority of patients undergoing (C)RT. In this review, we tried to understand what are the main areas in which interventions can be made prior to the (C)RT start, the possible side effects of the treatment, the effectiveness in their prevention and management, and the impact that prehabilitation may have in adherence to therapy and on the principal survival outcomes, providing important guidance for the planning of future studies.
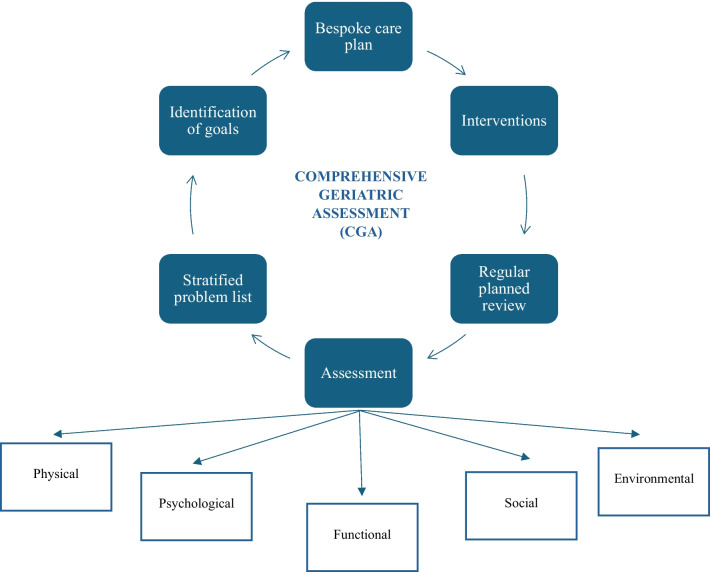
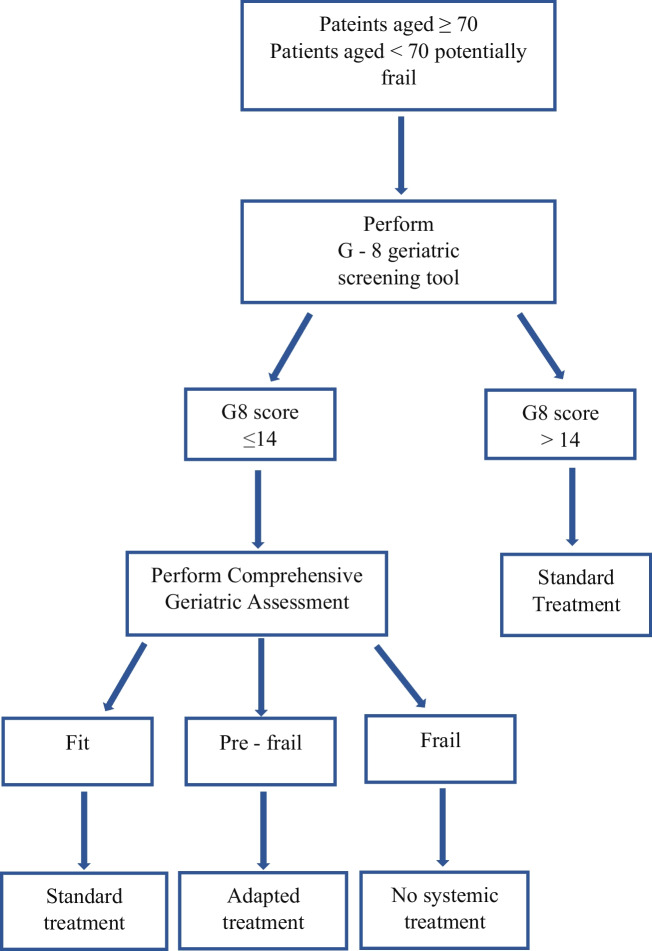
Evidences and conclusions: Although there is no strong data evaluating multidisciplinary prehabilitation strategies, evidence shows that optimizing the patient's health status and preventing possible complications improve the QoL, reduce the incidence and severity of adverse events, and improve treatment adherence. While cardiology prehabilitation is of paramount importance for all patients undergoing concomitant CRT in the prevention of possible side effects, the remaining interventions are useful independently of the type of treatment proposed. Geriatricians have a key role in both elderly patients and younger patients characterized by many comorbidities to comprehensively assess health status and indicate which treatment may be the best in terms of risk/benefit ratio. Collaboration between nutritionists and phoniatrics, on the other hand, ensures adequate nutritional intake for the patient, where possible orally. This is because optimizing both body weight and muscle mass and qualities has been shown to impact key survival outcomes. Finally, HNSCC patients have the second highest suicide rate, and the disease has side effects such as pain, dysfiguration, and sialorrhea that can reduce the patient's social life and create shame and embarrassment: A psychological intake, in addition to the usefulness to the patient, can also provide current support to caregivers and family members. Therefore clinicians must define a personalized pathway for patients, considering the characteristics of the disease and the type of treatment proposed, to optimize health status and prevent possible side effects while also improving QoL and treatment adherence.
Keywords: Head and neck squamous cell carcinoma; Prehabilitation; QoL.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Leemans CR, Braakhuis BJM, Brakenhoff RH (2011) The molecular biology of head and neck cancer. Nat Rev Cancer 11(1):9–22. 10.1038/nrc2982 - PubMed
-
- Sung H, Ferlay J, Siegel RL et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin 71(3):209–249. 10.3322/caac.21660 - PubMed
-
- Ferlay J, Colombet M, Soerjomataram I et al (2019) Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer 144(8):1941–1953. 10.1002/ijc.31937 - PubMed
-
- Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Allen C, et al. (2017) Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol 3(4):524. 10.1001/jamaoncol.2016.5688 - PMC - PubMed
-
- Noronha V, Joshi A, Patil VM et al (2018) Once-a-week versus once-every-3-weeks cisplatin chemoradiation for locally advanced head and neck cancer: a phase iii randomized noninferiority trial. JCO 36(11):1064–1072. 10.1200/JCO.2017.74.9457 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
