

Neonatal encephalopathy due to suspected hypoxic ischemic encephalopathy: pathophysiology, current, and emerging treatments
- PMID: 39237728
- PMCID: PMC11582131
- DOI: 10.1007/s12519-024-00836-9
Neonatal encephalopathy due to suspected hypoxic ischemic encephalopathy: pathophysiology, current, and emerging treatments
Abstract
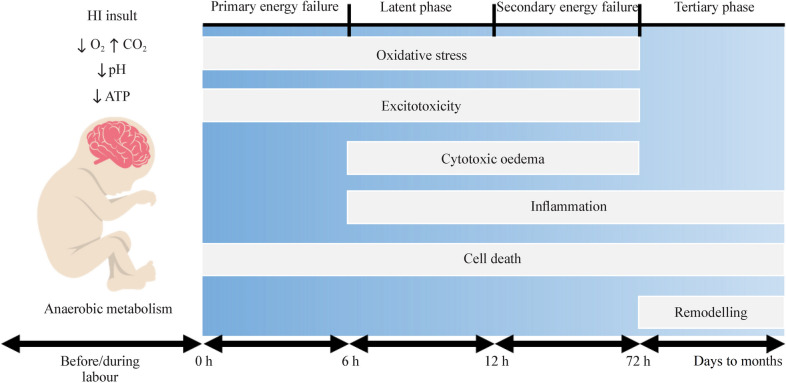
Background: Neonatal encephalopathy (NE) due to suspected hypoxic-ischemic encephalopathy (HIE), referred to as NESHIE, is a clinical diagnosis in late preterm and term newborns. It occurs as a result of impaired cerebral blood flow and oxygen delivery during the peripartum period and is used until other causes of NE have been discounted and HIE is confirmed. Therapeutic hypothermia (TH) is the only evidence-based and clinically approved treatment modality for HIE. However, the limited efficacy and uncertain benefits of TH in some low- to middle-income countries (LMICs) and the associated need for intensive monitoring have prompted investigations into more accessible and effective stand-alone or additive treatment options.
Data sources: This review describes the rationale and current evidence for alternative treatments in the context of the pathophysiology of HIE based on literatures from Pubmed and other online sources of published data.
Results: The underlining mechanisms of neurotoxic effect, current clinically approved treatment, various categories of emerging treatments and clinical trials for NE are summarized in this review. Melatonin, caffeine citrate, autologous cord blood stem cells, Epoetin alfa and Allopurinal are being tested as potential neuroprotective agents currently.
Conclusion: This review describes the rationale and current evidence for alternative treatments in the context of the pathophysiology of HIE. Neuroprotective agents are currently only being investigated in high- and middle-income settings. Results from these trials will need to be interpreted and validated in LMIC settings. The focus of future research should therefore be on the development of inexpensive, accessible monotherapies and should include LMICs, where the highest burden of NESHIE exists.
Keywords: Brain; Cerebrovascular circulation; Hypoxia–ischemia; Induced hypothermia; Neuroprotective agents.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. Ethical approval: Not applicable.
Figures
References
-
- Executive summary: Neonatal encephalopathy and neurologic outcome, second edition. Report of the American college of obstetricians and gynecologists’ task force on neonatal encephalopathy. Obstet Gynecol. 2014;123:896–901. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
