

An actinomycosis infection resembling peritoneal dissemination of rectal cancer: a case report
- PMID: 39237794
- PMCID: PMC11377367
- DOI: 10.1186/s40792-024-02005-6
An actinomycosis infection resembling peritoneal dissemination of rectal cancer: a case report
Abstract
Background: Actinomycosis is a suppurative and granulomatous inflammation commonly caused by Actinomyces israelii. Due to its rarity and the paucity of characteristic clinical features, diagnosis of intra-abdominal actinomycosis is challenging, especially when the patient has a treatment history of abdominal cancer.
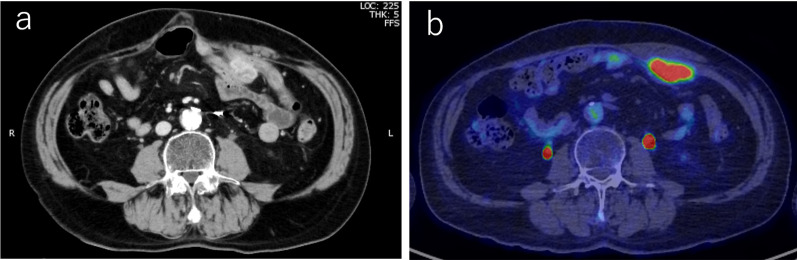
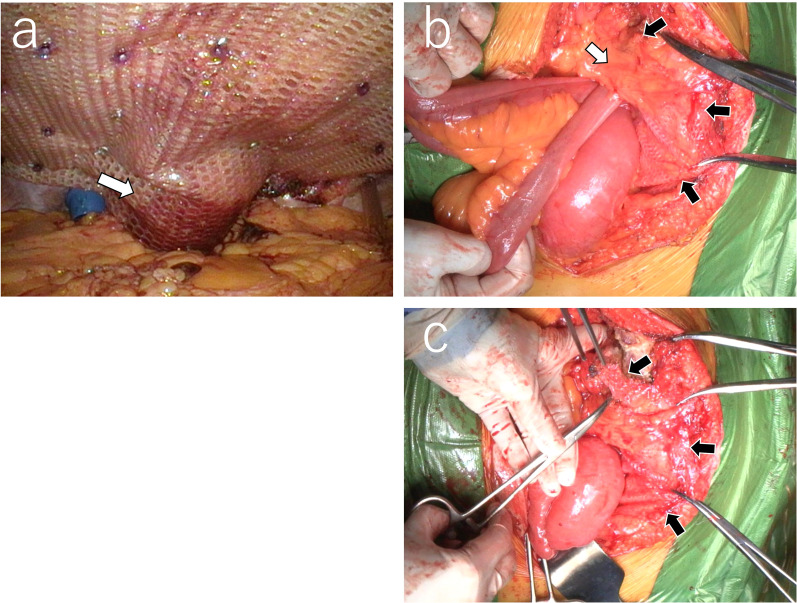
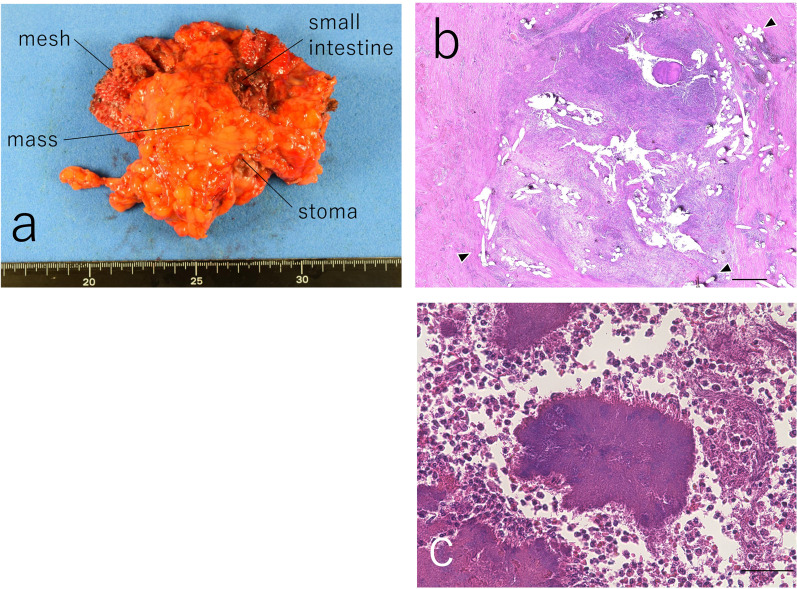
Case presentation: The patient is a 72-year-old man who has a history of multiple abdominal surgeries for rectal cancer, including low anterior resection for primary rectal cancer, partial hepatic resection for metachronous liver metastasis, and Hartmann surgery for local recurrence. The patient has also undergone parastomal hernia repair using the Sugarbaker method. One year after hernia repair, computed tomography (CT) identified a mass lesion between the abdominal wall and the mesh, suggesting the possibility of peritoneal recurrence of rectal cancer. The accumulation of fluorodeoxyglucose (FDG) was evident via positron emission tomography-CT (PET-CT), while tumor marker levels were within the normal range. On laparotomy, the small intestine, abdominal wall, mesh, colon, and stoma were observed to be associated with the mass lesion, and en bloc resection was carried out. However, postoperative histopathological examination revealed an actinomyces infection without any cancerous cells.
Conclusions: This case highlights the challenges faced by surgeons regarding preoperative diagnosis of actinomycosis, especially when it occurs after the resection of abdominal cancer. Also, this case reminds us of the importance of a histopathological examination for abdominal masses or nodules before starting chemotherapy.
Keywords: Abdominal actinomycosis; Hernia; Mesh; Peritoneal dissemination.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
