

Interrelationships among metabolic syndrome, bone-derived cytokines, and the most common metabolic syndrome-related diseases negatively affecting bone quality
- PMID: 39238022
- PMCID: PMC11378428
- DOI: 10.1186/s13098-024-01440-7
Interrelationships among metabolic syndrome, bone-derived cytokines, and the most common metabolic syndrome-related diseases negatively affecting bone quality
Abstract
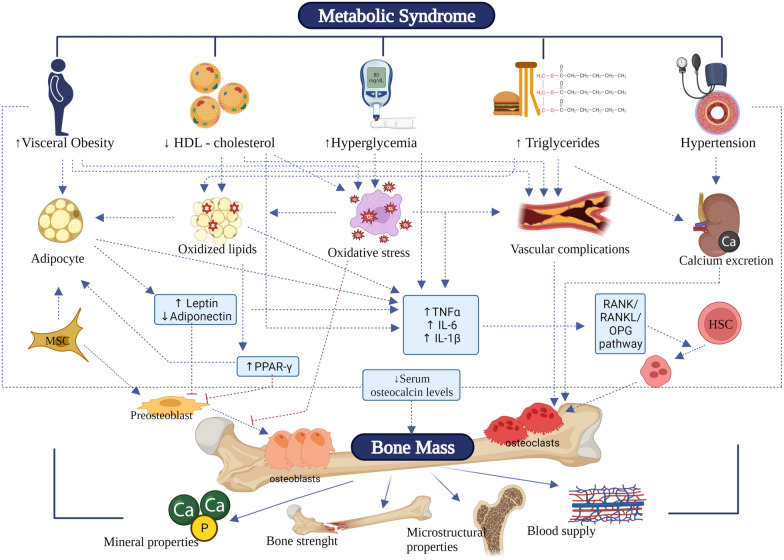
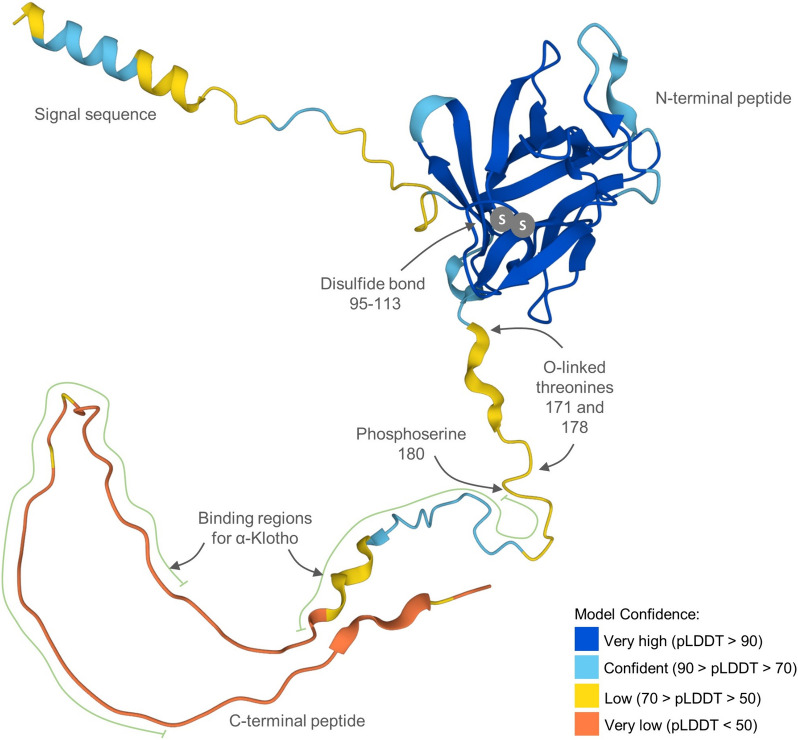
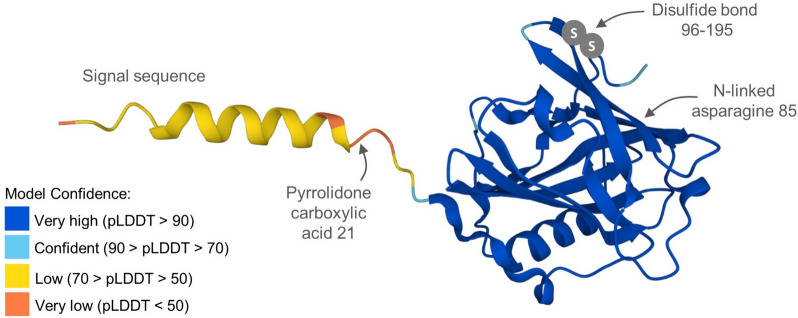
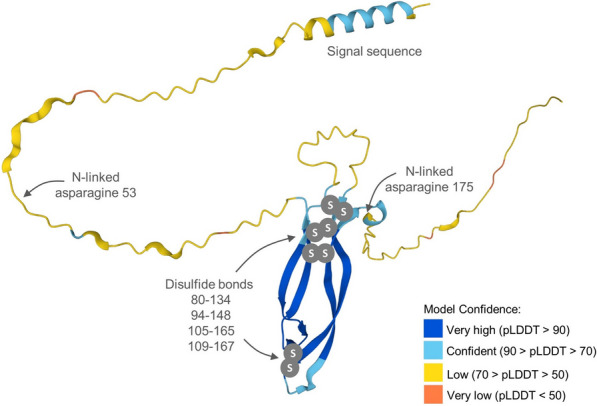
Metabolic syndrome (MetS), as a set of medical conditions including hyperglycemia, hypertension, abdominal obesity, and dyslipidemia, represents a highly prevalent disease cluster worldwide. The individual components of MetS together increase the risk of MetS-related disorders. Recent research has demonstrated that bone, as an endocrine organ, releases several systemic cytokines (osteokines), including fibroblast growth factor 23 (FGF23), lipocalin 2 (LCN2), and sclerostin (SCL). This review not only summarizes current knowledge about MetS, osteokines and the most common MetS-related diseases with a detrimental impact on bone quality (type 2 diabetes mellitus: T2DM; cardiovascular diseases: CVDs; osteoporosis: OP), but also provides new interpretations of the relationships between osteokines and individual components of MetS, as well as between osteokines and MetS-related diseases mentioned above. In this context, particular emphasis was given on available clinical studies. According to the latest knowledge, FGF23 may become a useful biomarker for obesity, T2DM, and CVDs, as FGF23 levels were increased in patients suffering from these diseases. LCN2 could serve as an indicator of obesity, dyslipidemia, T2DM, and CVDs. The levels of LCN2 positively correlated with obesity indicators, triglycerides, and negatively correlated with high-density lipoprotein (HDL) cholesterol. Furthermore, subjects with T2DM and CVDs had higher LCN2 levels. SCL may act as a potential biomarker predicting the incidence of MetS including all its components, T2DM, CVDs, and OP. Elevated SCL levels were noted in individuals with T2DM, CVDs and reduced in patients with OP. The aforementioned bone-derived cytokines have the potential to serve as promising predictors and prospective treatment targets for MetS and MetS-related diseases negatively affecting bone quality.
Keywords: Bone health; Cardiovascular diseases; Fibroblast growth factor 23; Lipocalin 2; Metabolic syndrome; Osteoporosis; Sclerostin; Type 2 diabetes mellitus.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120:1640–5. 10.1161/CIRCULATIONAHA.109.192644 - DOI - PubMed
-
- Noubiap JJ, Nansseu JR, Lontchi-Yimagou E, Nkeck JR, Nyaga UF, Ngouo AT, et al. Geographic distribution of metabolic syndrome and its components in the general adult population: a meta-analysis of global data from 28 million individuals. Diabetes Res Clin Pract. 2022;188:109924. 10.1016/j.diabres.2022.109924 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
