

Stevens-Johnson syndrome and toxic epidermal necrolysis: Updates in pathophysiology and management
- PMID: 39238098
- PMCID: PMC11441865
- DOI: 10.1097/CM9.0000000000003250
Stevens-Johnson syndrome and toxic epidermal necrolysis: Updates in pathophysiology and management
Abstract
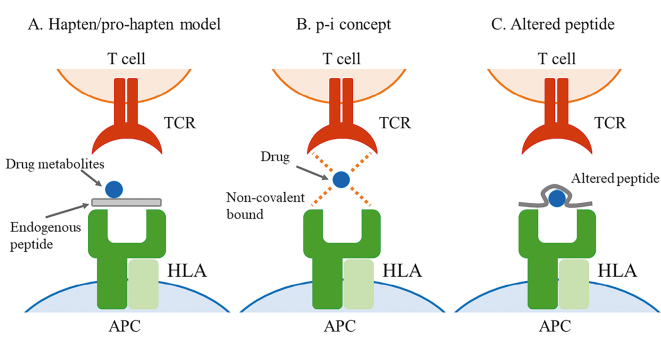
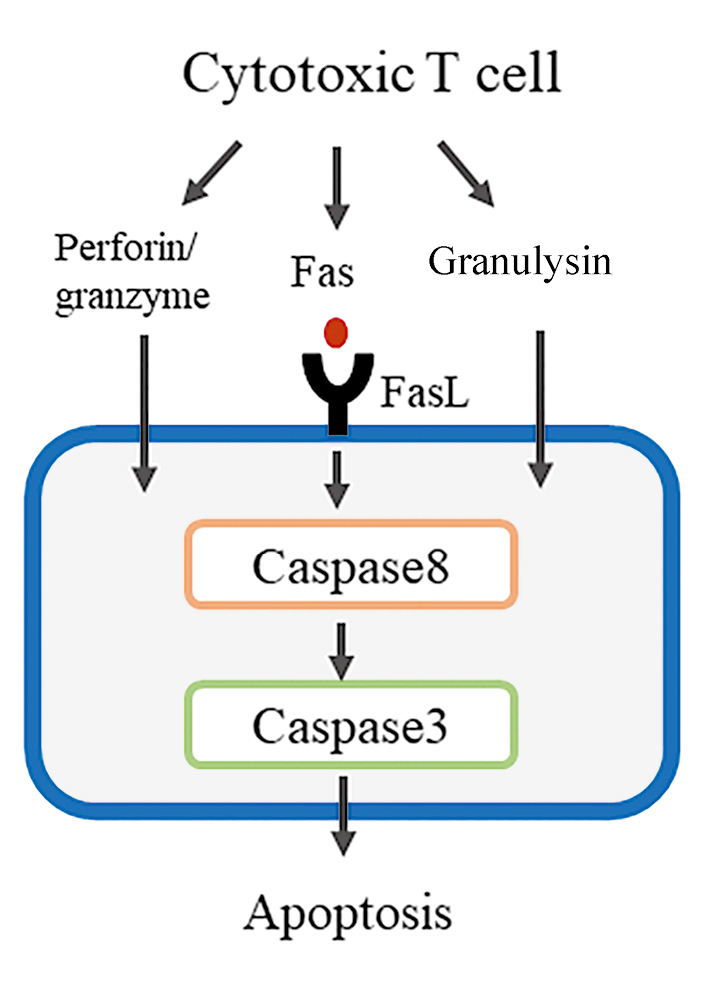
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are life-threatening conditions characterized by extensive detachment of the epidermis and mucous membranes. These severe disorders carry a high mortality rate, and their pathogenesis remains largely unclear. Furthermore, optimal therapeutic strategies for SJS/TEN remain a subject of ongoing debate. Early diagnosis of SJS/TEN is challenging, and reliable biomarkers for diagnosis or severity prediction have not been firmly established. Certain drugs, such as carbamazepine and allopurinol, have shown a strong association with specific human leukocyte antigen (HLA) types. Recently, the potential benefits of HLA screening prior to administering these drugs to reduce the incidence of SJS/TEN have been explored. Epidermal cell death in SJS/TEN lesions is caused by extensive apoptosis, primarily through the Fas-Fas ligand (FasL) and perforin/granzyme pathways. Our findings suggest that necroptosis, a form of programmed necrosis, also contributes to epidermal cell death. Annexin A1, released from monocytes, interacts with the formyl peptide receptor 1 to induce necroptosis. Several biomarkers, such as CC chemokine ligand (CCL)-27, interleukin-15, galectin-7, receptor-interacting protein kinases 3 (RIP3), and lipocalin-2, have been identified for diagnostic and prognostic purposes in SJS/TEN. Supportive care is recommended for treating SJS/TEN, but the efficacy of various therapeutic options-including systemic corticosteroids, intravenous immunoglobulin, cyclosporine, and tumor necrosis factor-α antagonists-remains controversial. Recent studies have investigated the potential benefits of tumor necrosis factor-α antagonists. In this review, we discuss recent advances in the understanding and management of SJS/TEN.
Copyright © 2024 The Chinese Medical Association, produced by Wolters Kluwer, Inc. under the CC-BY-NC-ND license.
Conflict of interest statement
None.
Figures



References
-
- Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol 1993;129:92–96. doi: 10.1001/archderm.1993.01680220104023. - PubMed
-
- Sunaga Y Kurosawa M Ochiai H Watanabe H Sueki H Azukizawa H, et al. The nationwide epidemiological survey of Stevens-Johnson syndrome and toxic epidermal necrolysis in Japan, 2016-2018. J Dermatol Sci 2020;100:175–182. doi: 10.1016/j.jdermsci.2020.09.009. - PubMed
-
- Revuz J Penso D Roujeau JC Guillaume JC Payne CR Wechsler J, et al. Toxic epidermal necrolysis. Clinical findings and prognosis factors in 87 patients. Arch Dermatol 1987;123:1160–1165. doi: 10.1001/archderm.123.9.1160. - PubMed
-
- Mockenhaupt M Viboud C Dunant A Naldi L Halevy S Bouwes Bavinck JN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: Assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR-study. J Invest Dermatol 2008;128:35–44. doi: 10.1038/sj.jid.5701033. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
