

Health workers' perspectives on the quality of maternal and newborn health care around the time of childbirth: Results of the Improving MAternal Newborn carE in the EURO Region (IMAgiNE EURO) project in 12 countries of the World Health Organization European Region
- PMID: 39238363
- PMCID: PMC11377968
- DOI: 10.7189/jogh.14.04164
Health workers' perspectives on the quality of maternal and newborn health care around the time of childbirth: Results of the Improving MAternal Newborn carE in the EURO Region (IMAgiNE EURO) project in 12 countries of the World Health Organization European Region
Abstract
Background: Health workers' (HWs') perspectives on the quality of maternal and newborn care (QMNC) are not routinely collected. In this cross-sectional study, we aimed to document HWs' perspectives on QMNC around childbirth in 12 World Health Organization (WHO) European countries.
Methods: HWs involved in maternal/neonatal care for at least one year between March 2020 and March 2023 answered an online validated WHO standards-based questionnaire collecting 40 quality measures for improving QMNC. A QMNC index (score 0-400) was calculated as a synthetic measure.
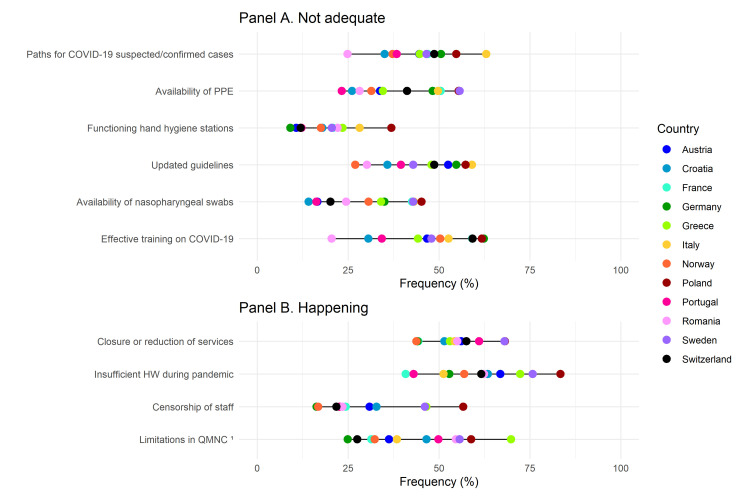
Results: Data from 4143 respondents were analysed. For 39 out of 40 quality measures, at least 20% of HWs reported a 'need for improvement', with large variations across countries. Effective training on healthy women/newborns management (n = 2748, 66.3%), availability of informed consent job aids (n = 2770, 66.9%), and effective training on women/newborns rights (n = 2714, 65.5%) presented the highest proportion of HWs stating 'need for improvement'. Overall, 64.8% (n = 2684) of respondents declared that HWs' numbers were insufficient for appropriate care (66.3% in Portugal and 86.6% in Poland), and 22.4% described staff censorship (16.3% in Germany and 56.7% in Poland). The reported QMNC index was low in all countries (Poland median (MD) = 210.60, interquartile range (IQR) = 155.71, 273.57; Norway MD = 277.86; IQR = 244.32, 308.30). The 'experience of care' domain presented in eight countries had significantly lower scores than the other domains (P < 0.001). Over time, there was a significant monthly linear decrease in the QMNC index (P < 0.001), lacking correlation with the coronavirus disease 2019 (COVID-19) pandemic trends (P > 0.05). Multivariate analyses confirmed large QMNC variation by country. HWs with <10 years of experience, HWs from public facilities, and midwives rated QMNC with significantly lower scores (P < 0.001).
Conclusions: HWs from 12 European countries reported significant gaps in QMNC, lacking association with COVID-19 pandemic trends. Routine monitoring of QMNC and tailored actions are needed to improve health services for the benefit of both users and providers.
Registration: ClinicalTrials.gov NCT04847336.
Copyright © 2024 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interests: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Figures






References
-
- World Health Organization. Promoting health through the life-course. Global Strategy for Women’s, Children's and Adolescent's Health 2016-2030. 2015. Available: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/g.... Accessed: 15 September 2023.
-
- United Nations. Sustainable Development Knowledge Platform. Transforming our World: The 2030 Agenda for sustainable development. 2015. Available: https://sdgs.un.org/2030agenda. Accessed: 15 September 2023.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
