

Behçet's Syndrome With Multiple Bilateral Pulmonary Aneurysms Associated With Endomyocardial Fibrosis Presented With Pulmonary Emboli: A Case Report
- PMID: 39238732
- PMCID: PMC11376314
- DOI: 10.7759/cureus.66281
Behçet's Syndrome With Multiple Bilateral Pulmonary Aneurysms Associated With Endomyocardial Fibrosis Presented With Pulmonary Emboli: A Case Report
Abstract
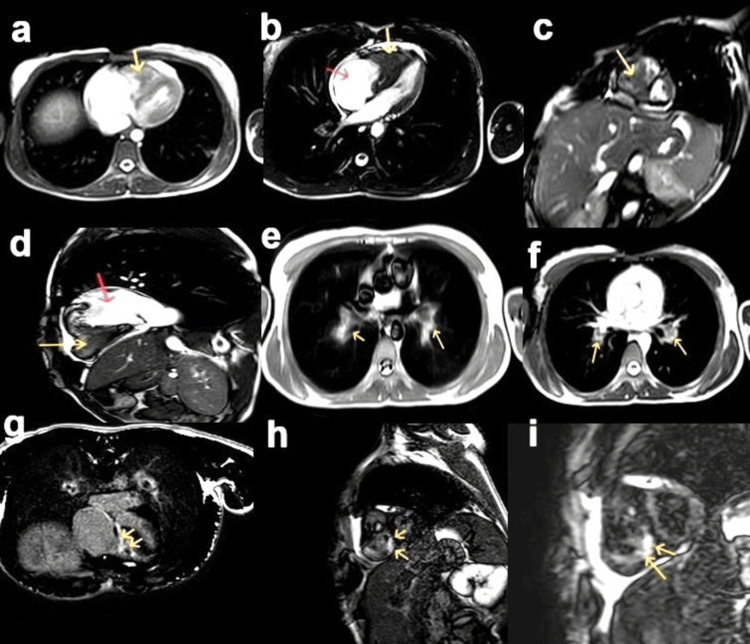
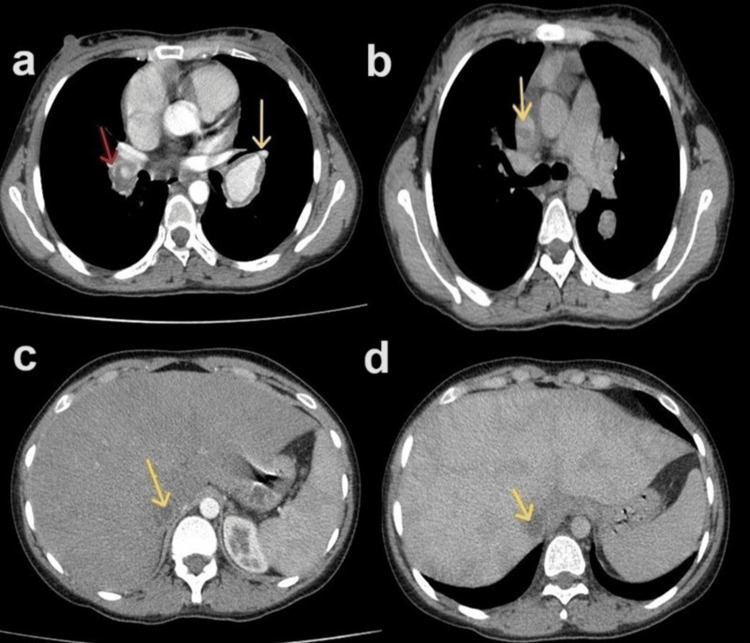
Behçet's syndrome (BS) is a rare chronic multisystemic inflammatory disorder of unknown etiopathogenesis. BS is classified as a vasculitis of variable vessel size, which can manifest in both arterial and venous blood vessels. BS commonly presents with mucocutaneous and ocular manifestations. Superficial and deep vein thrombosis is present in 50% of patients, with atypical venous thrombosis affecting the inferior vena cava, superior vena cava, hepatic veins with Budd-Chiari syndrome, portal vein, cerebral sinuses, and right atrium and ventricle. Arterial manifestations include in situ thrombosis, pulmonary artery aneurysms, aneurysms of the abdominal aorta, and aneurysms of visceral and peripheral arteries. This article reports a new case of BS in a 28-year-old female patient who presented with severe dyspnea and hemoptysis. Echocardiography and cardiovascular magnetic resonance imaging led to the diagnosis of endomyocardial fibrosis and a large right ventricular thrombus with pulmonary embolism. Computed tomography angiography revealed multiple pulmonary aneurysms and emboli. Rare findings such as endomyocardial fibrosis and Budd-Chiari syndrome were noted. This case highlights the role of medical imaging modalities in diagnosing rare syndromes such as BS, as demonstrated in the current case.
Keywords: behçet's syndrome; budd-chiari syndrome; endomyocardial fibrosis; hughes-stovin syndrome; multiple pulmonary artery aneurysms; pulmonary artery thrombosis.
Copyright © 2024, Almutamaiz et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Behçet's syndrome. Emmi G, Bettiol A, Hatemi G, Prisco D. Lancet. 2024;16:1093–1108. - PubMed
-
- Behçet: the syndrome. Bettiol A, Prisco D, Emmi G. Rheumatology (Oxford) 2020;59:0–7. - PubMed
-
- Behcet's disease: epidemiology, clinical manifestations, and diagnosis. Davatchi F, Chams-Davatchi C, Shams H, et al. Expert Rev Clin Immunol. 2017;13:57–65. - PubMed
-
- An update on Behçet's syndrome. (Article in German) Xenitidis T, Henes JC. Dtsch Med Wochenschr. 2023;148:1129–1134. - PubMed
-
- Vascular Behçet syndrome: from pathogenesis to treatment. Bettiol A, Alibaz-Oner F, Direskeneli H, et al. Nat Rev Rheumatol. 2023;19:111–126. - PubMed
Publication types
LinkOut - more resources
Full Text Sources