

Development of the first Iranian clinical practice guidelines for the diagnosis, treatment, and secondary prevention of acute coronary syndrome
- PMID: 39239072
- PMCID: PMC11376720
- DOI: 10.4103/jrms.jrms_851_23
Development of the first Iranian clinical practice guidelines for the diagnosis, treatment, and secondary prevention of acute coronary syndrome
Abstract
Background: This article introduces the first national guidelines for the management including diagnosis, treatment, and secondary prevention of acute coronary syndrome (ACS) in Iran.
Materials and methods: The members of the guideline development group (GDG) were specialists and experts in fields related to ACS and were affiliated with universities of medical sciences or scientific associations in the country. They carefully examined the evidence and clinical concerns related to ACS management and formulated 13 clinical questions that were sent to systematic review group who developed related evidence using Grade method. Finally the GDG developed the recommendations and suggestions of the guideline.
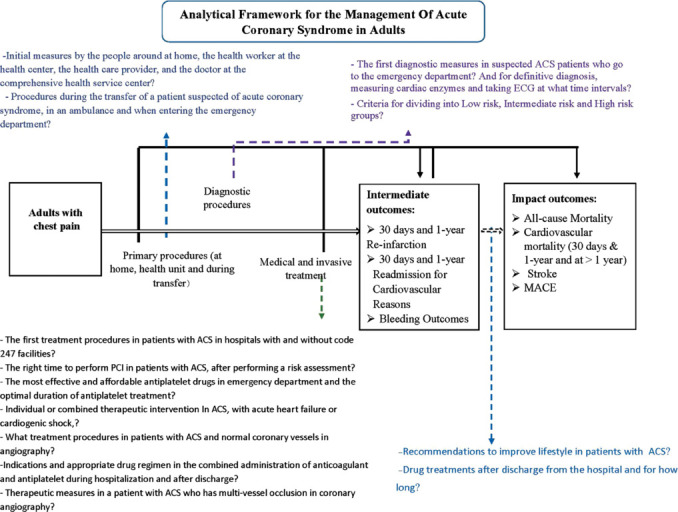
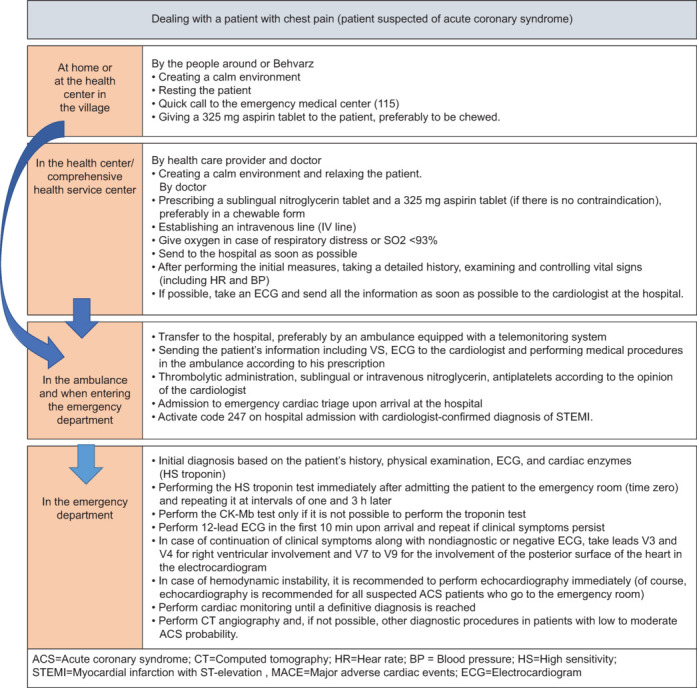
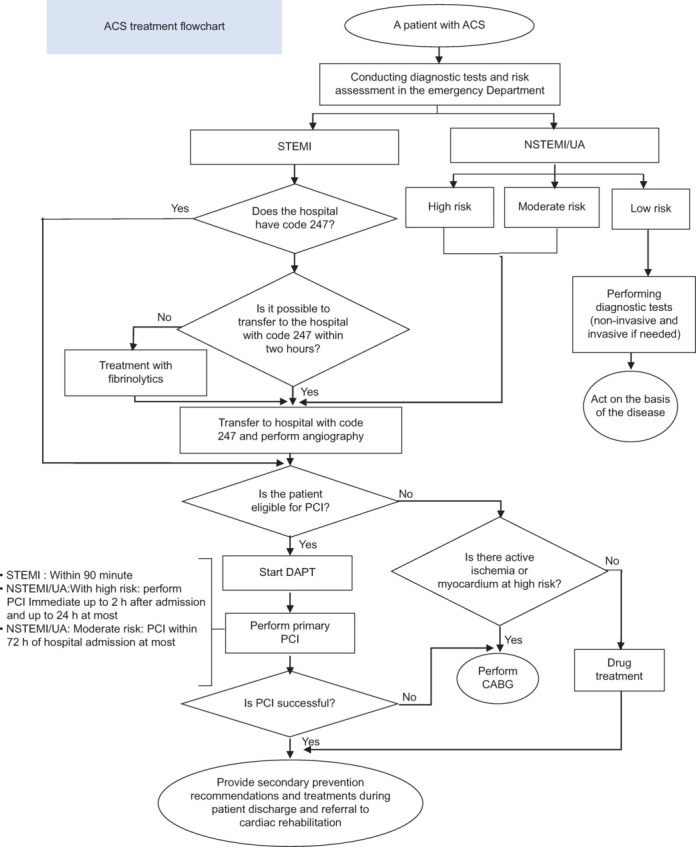
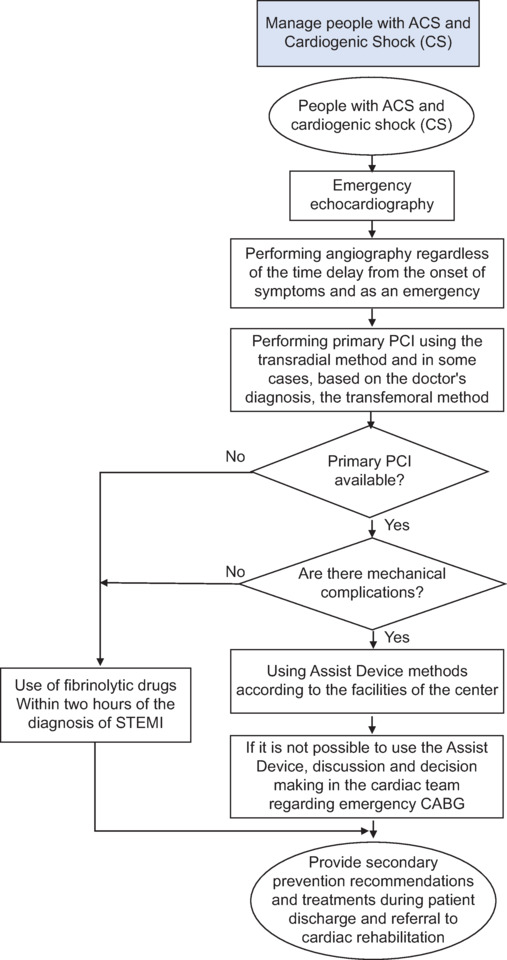
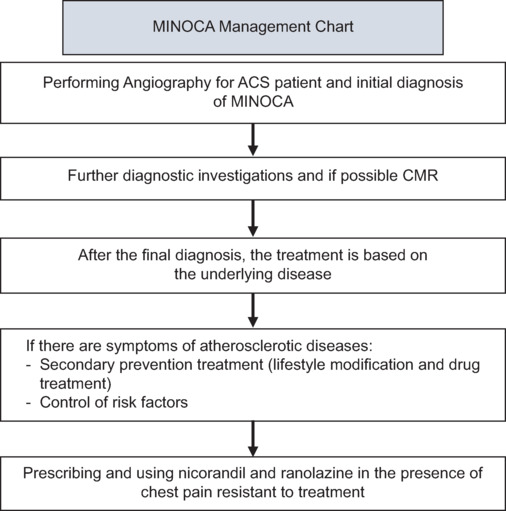
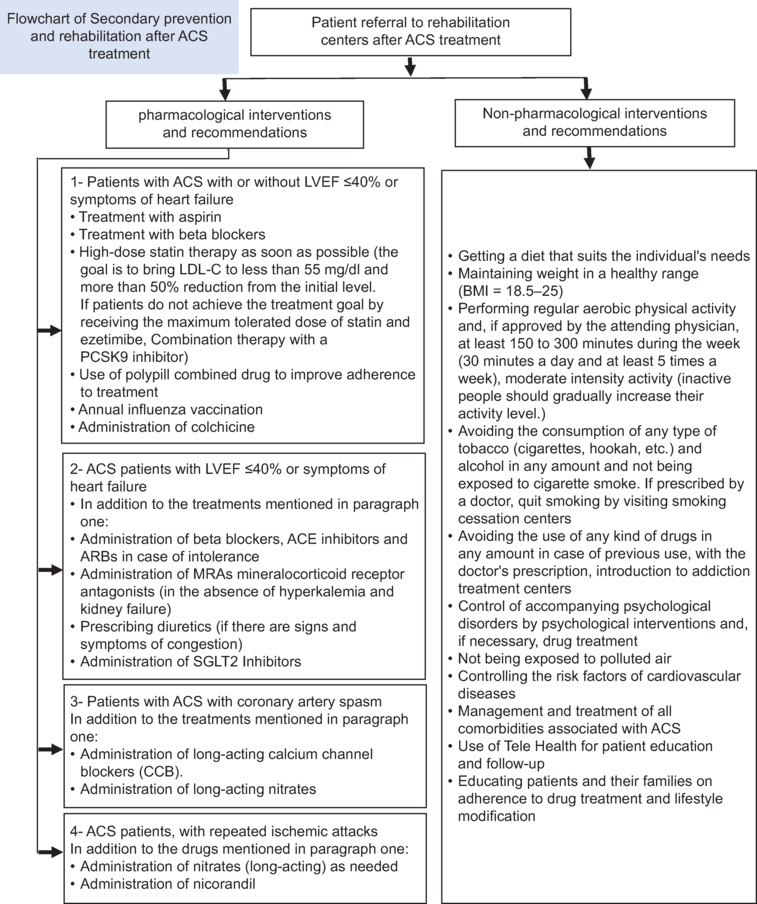
Results: The first three questions in the guideline focus on providing recommendations for handling a patient who experience chest pain at home, in a health house or center, during ambulance transportation, and upon arrival at the emergency department (ED) as well as the initial diagnostic measures in the ED. Subsequently, the recommendations related to the criteria for categorizing patients into low, intermediate and high-risk groups are presented. The guideline addressed primary treatment measures for ACS patients in hospitals with and without code 247 or having primary percutaneous coronary intervention (PCI) facilities, and the appropriate timing for PCI based on the risk assessment. In addition, the most efficacious antiplatelet medications for ACS patients in the ED as well as its optimal duration of treatment are presented. The guideline details the recommendations for therapeutic interventions in patients with ACS and acute heart failure, cardiogenic shock, myocardial infarction with nonobstructive coronary arteries (MINOCA), multivessel occlusion, as well as the indication for prescribing a combined use of anticoagulants and antiplatelet during hospitalization and upon discharge. Regarding secondary prevention, while emphasizing the referral of these patients to rehabilitation centers, other interventions that include pharmaceutical and nonpharmacological ones are addressed, In addition, necessary recommendations for enhancing lifestyle and posthospital discharge pharmaceutical treatments, including their duration, are provided. There are specific recommendations and suggestions for subgroups, such as patients aged over 75 years and individuals with heart failure, diabetes, and chronic kidney disease.
Conclusion: Developing guidelines for ACS diagnosis, treatment and secondary prevention according to the local context in Iran can improve the adherence of our health care providers, patients health, and policy makers plans.
Keywords: Acute coronary syndrome; ST-elevation myocardial infarction; clinical practice guideline; non-ST-elevation myocardial infarction; unstable angina.
Copyright: © 2024 Journal of Research in Medical Sciences.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Norouzzadeh R, Heidari M. Predicting the risk of acute coronary syndrome in the elderly based on reported symptoms. Feyz J Kashan Univ Med Sci. 2013:16.
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al. 2014 AHA/ACC guideline for the management of patients with non – ST-elevation acute coronary syndromes: A report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014;64:e139–e228. - PubMed
-
- Li YH, Wang YC, Wang YC, Liu JC, Lee CH, Chen CC, et al. 2018 Guidelines of the Taiwan Society of Cardiology, Taiwan Society of Emergency Medicine and Taiwan Society of Cardiovascular Interventions for the management of non ST-segment elevation acute coronary syndrome. J Formos Med Assoc. 2018;117:766–90. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous