

Atrial Fibrillation as a Prognostic Factor for All-Cause Mortality in Patients With Transthyretin Amyloid Cardiomyopathy
- PMID: 39239341
- PMCID: PMC11371936
- DOI: 10.1016/j.jaccao.2024.03.007
Atrial Fibrillation as a Prognostic Factor for All-Cause Mortality in Patients With Transthyretin Amyloid Cardiomyopathy
Abstract
Background: Atrial fibrillation/atrial flutter (AF/AFL) are common manifestations of transthyretin amyloid cardiomyopathy (ATTR-CM) but have not been found to be predictive of mortality.
Objectives: This analysis aimed to examine whether baseline or historical AF/AFL at enrollment was prognostic for all-cause mortality.
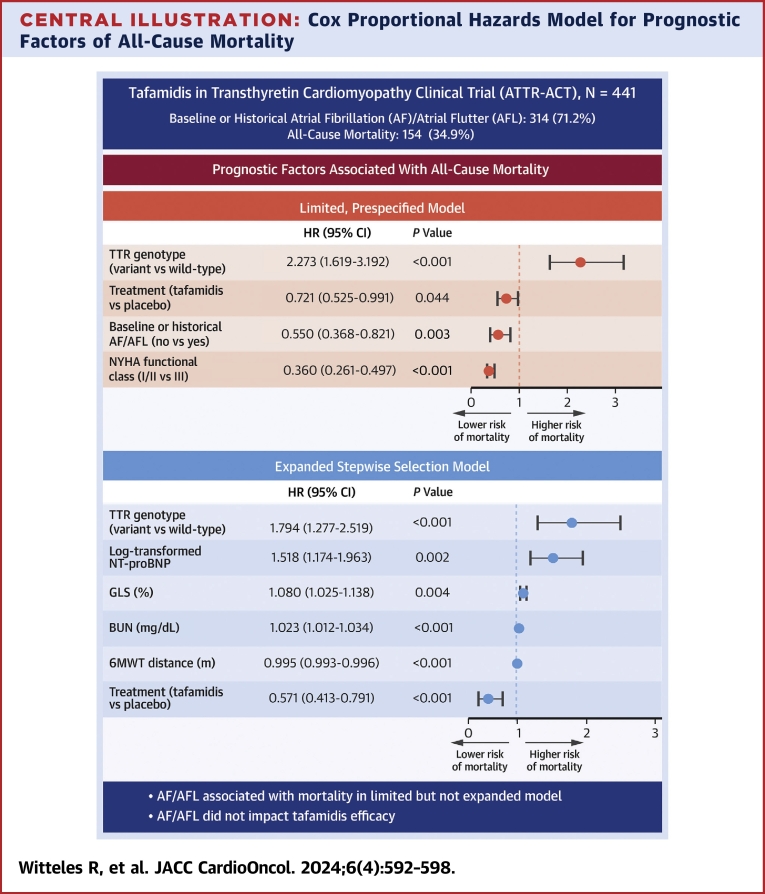
Methods: In the ATTR-ACT (Tafamidis in Transthyretin Cardiomyopathy Clinical Trial), a 30-month study of tafamidis vs placebo for ATTR-CM, AF/AFL was evaluated as an independent prognostic factor for all-cause mortality using Cox proportional hazards modelling. The impact of AF/AFL on tafamidis efficacy was explored by adding an interaction term for AF/AFL status and treatment.
Results: ATTR-ACT enrolled 441 patients with ATTR-CM (median age 75 years; 90% male); 314 (71.2%) had baseline or historical AF/AFL at enrollment. AF/AFL was an independent prognostic factor for all-cause mortality after adjusting for covariates prespecified in the ATTR-ACT model (treatment, genotype, New York Heart Association functional class; HR: 0.550; 95% CI: 0.368-0.821) but not in an expanded stepwise model selection analysis including 23 covariates (blood urea nitrogen and N-terminal pro-B-type natriuretic peptide concentration, 6-minute walk test distance, genotype, treatment, and global longitudinal strain were prognostic [P < 0.01]). The interactions between tafamidis treatment and AF/AFL for all-cause mortality (P = 0.33) and changes in Kansas City Cardiomyopathy Questionnaire Overall Summary score (P = 0.83) and 6-minute walk test distance (P = 0.82) were not significant.
Conclusions: In ATTR-ACT, baseline or historical AF/AFL was prognostic for all-cause mortality in analyses with limited adjustment but not after accounting for additional indicators of disease severity. Baseline or historical AF/AFL did not impact the efficacy of tafamidis treatment. (Safety and Efficacy of Tafamidis in Patients With Transthyretin Cardiomyopathy [ATTR-ACT]; NCT01994889).
Keywords: amyloidosis; arrhythmia; cardiomyopathy; heart failure.
© 2024 The Authors.
Conflict of interest statement
Dr Witteles has received honoraria for advisory board participation from Alnylam, AstraZeneca, BridgeBio, Eidos, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer; and funding for clinical trials from Alnylam, BridgeBio, Ionis, Janssen, and Pfizer. Dr Kapa has served on an advisory board for Pfizer. Dr Cappelli has received honoraria for advisory board participation from Akcea, Alnylam, Novo Nordisk, and Pfizer; and his institution has received an unconditional research grant from Pfizer. Dr Sultan and Mr Gundapaneni are current or former employees of Pfizer; and hold stock/stock options in Pfizer. Dr Davis has received honoraria for advisory board participation from Akcea, Alnylam, AstraZeneca, Bayer, Boehringer Ingelheim, Ferring, Ionis, Janssen, and Pfizer; consulting fees from Janssen and Novo Nordisk; speaker fees from Bayer, Ferring, Janssen, and Pfizer; and research funding from Pfizer. Dr Garcia-Pavia has served as a speaker in scientific meetings for Alnylam, BridgeBio, Ionis/AstraZeneca, and Pfizer; has received funding from Alnylam and Pfizer for scientific meeting expenses; has received consultancy fees from Alexion, Alnylam, AstraZeneca, Attralus, BridgeBio, Intellia, Neurimmune, Novo Nordisk, and Pfizer; and his institution has received research grants/educational support from Alnylam, AstraZeneca, BridgeBio, Intellia, Novo Nordisk, and Pfizer. Dr Jefferies has reported that he has no relationships relevant to the contents of this paper to disclose. Upon request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions and exceptions, Pfizer may also provide access to the related individual deidentified participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
Figures

References
-
- Kittleson M.M., Maurer M.S., Ambardekar A.V., et al. American Heart Association Heart Failure Transplantation Committee of the Council on Clinical Cardiology Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American Heart Association. Circulation. 2020;142(1):e7–e22. - PubMed
-
- Witteles R.M., Bokhari S., Damy T., et al. Screening for transthyretin amyloid cardiomyopathy in everyday practice. J Am Coll Cardiol HF. 2019;7(8):709–716. - PubMed
-
- Donnellan E., Wazni O.M., Hanna M., et al. Atrial fibrillation in transthyretin cardiac amyloidosis: predictors, prevalence, and efficacy of rhythm control strategies. J Am Coll Cardiol EP. 2020;6(9):1118–1127. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
