

Predictive Performance of Cardiovascular Risk Scores in Cancer Survivors From the UK Biobank
- PMID: 39239345
- PMCID: PMC11372025
- DOI: 10.1016/j.jaccao.2024.05.015
Predictive Performance of Cardiovascular Risk Scores in Cancer Survivors From the UK Biobank
Abstract
Background: Cardiovascular preventive strategies are guided by risk scores with unknown validity in cancer cohorts.
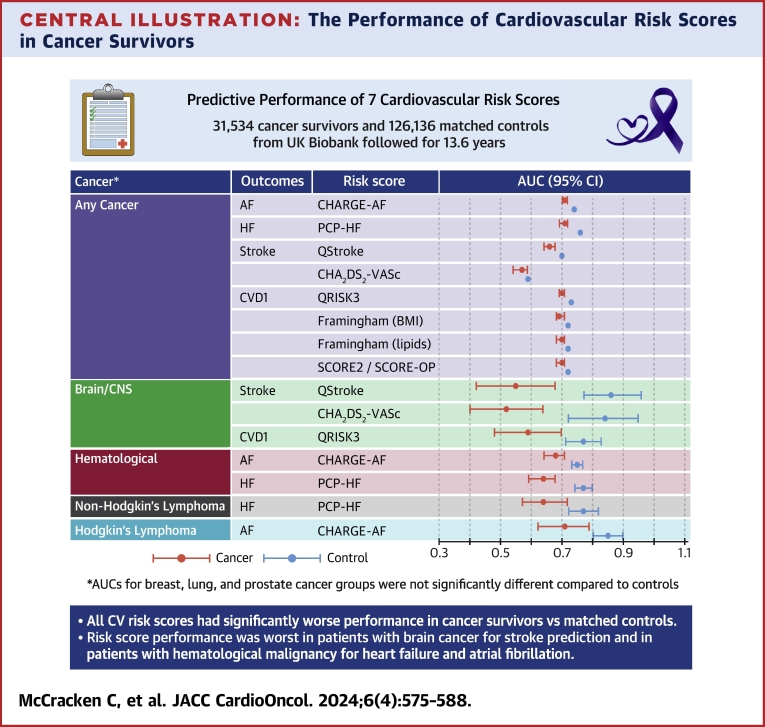
Objectives: This study aimed to evaluate the predictive performance of 7 established cardiovascular risk scores in cancer survivors from the UK Biobank.
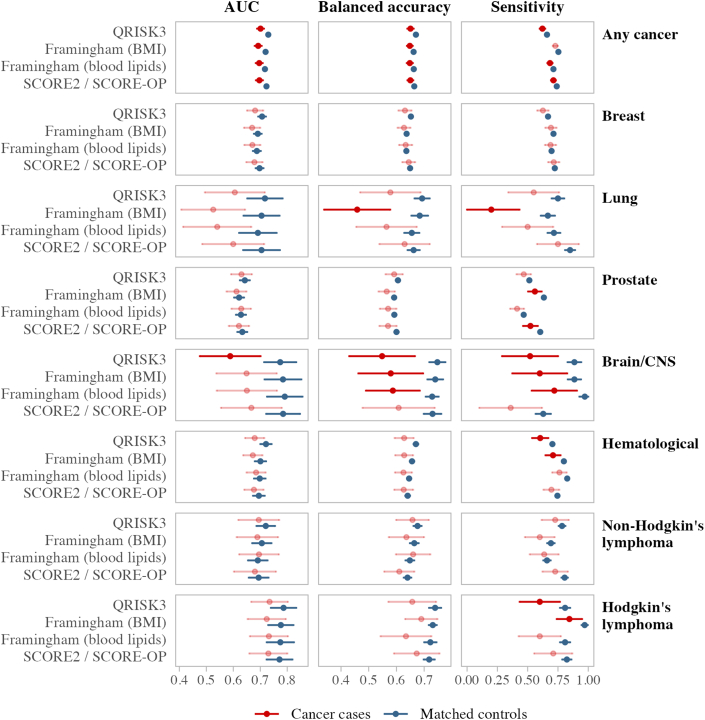
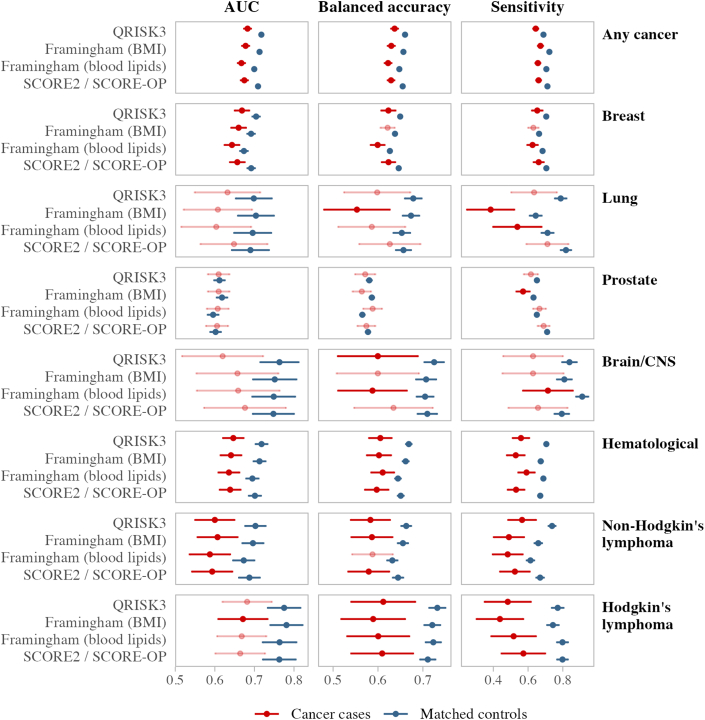
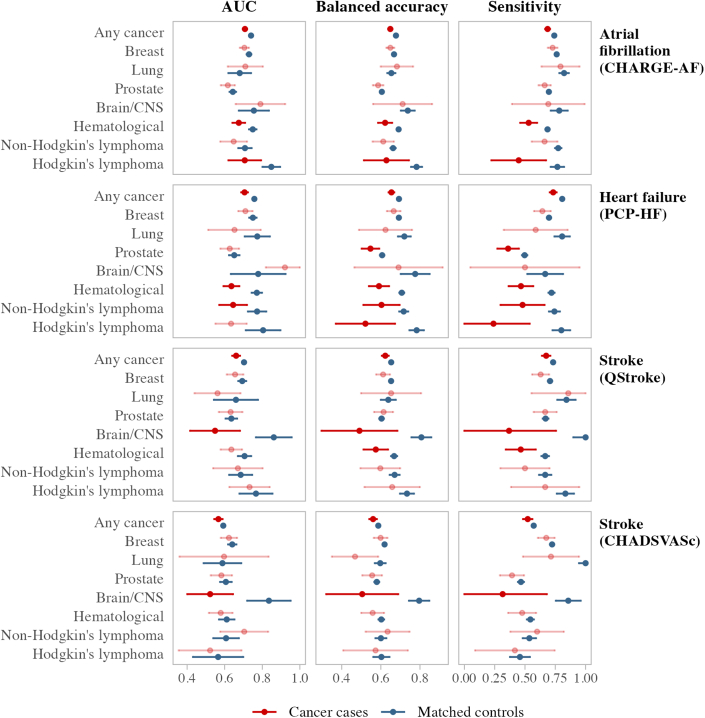
Methods: The predictive performance of QRISK3, Systematic Coronary Risk Evaluation 2 (SCORE2)/Systematic Coronary Risk Evaluation for Older Persons (SCORE-OP), Framingham Risk Score, Pooled Cohort equations to Prevent Heart Failure (PCP-HF), CHARGE-AF, QStroke, and CHA2DS2-VASc was calculated in participants with and without a history of cancer. Participants were propensity matched on age, sex, deprivation, health behaviors, family history, and metabolic conditions. Analyses were stratified into any cancer, breast, lung, prostate, brain/central nervous system, hematologic malignancies, Hodgkin lymphoma, and non-Hodgkin lymphoma. Incident cardiovascular events were tracked through health record linkage over 10 years of follow-up. The area under the receiver operating curve, balanced accuracy, and sensitivity were reported.
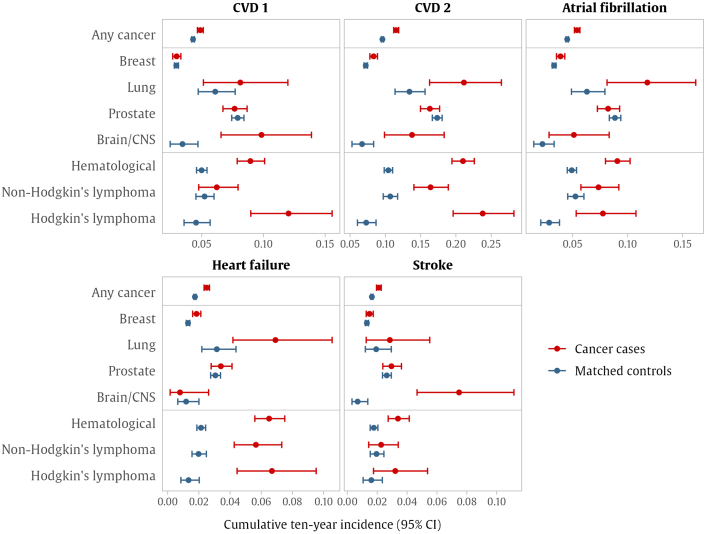
Results: The analysis included 31,534 cancer survivors and 126,136 covariate-matched controls. Risk score distributions were near identical in cases and controls. Participants with any cancer had a significantly higher incidence of all cardiovascular outcomes than matched controls. Performance metrics were significantly worse for all risk scores in cancer cases than in matched controls. The most notable differences were among participants with a history of hematologic malignancies who had significantly higher outcome rates and poorer risk score performance than their matched controls. The performance of risk scores for predicting stroke in participants with brain/central nervous system cancer was very poor, with predictive accuracy more than 30% lower than noncancer controls.
Conclusions: Existing cardiovascular risk scores have significantly worse predictive accuracy in cancer survivors compared with noncancer comparators, leading to an underestimation of risk in this cohort.
Keywords: cancer survivors; cardio-oncology; cardiovascular risk score; cohort studies; preventive medicine.
© 2024 The Authors.
Conflict of interest statement
Dr McCracken and Prof Neubauer are supported by the Oxford National Institute for Health and Care Research Biomedical Research Centre (IS-BRC-1215-20008). Prof Neubauer is additionally supported by the Oxford British Heart Foundation Centre of Research Excellence. Drs Condurache (G-002530) and Szabo (G-002389) were supported by the Barts Charity. This work was supported by the National Institute for Health and Care Research Barts Biomedical Research Centre (NIHR203330), a delivery partnership of Barts Health NHS Trust, Queen Mary University of London, St George’s University Hospitals NHS Foundation Trust and St George’s University of London. Dr Szabo and Prof Petersen have received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement no. 825903 (euCanSHare project). Prof Walter is codirector of the CanTest Collaborative, which is funded by Cancer Research UK (CC8640/A23385). Prof Mead is funded by a CRUK Senior Cancer Research Fellowship (grant number C42639/A26988). Prof Manisty is supported directly and indirectly from the National Institute for Health and Care Research Biomedical Research Centres at University College London Hospitals and Barts Health NHS Trusts. Prof Harvey is supported by the UK Medical Research Council (MC_PC_21003; MC_PC_21001) and National Institute for Health and Care Research Southampton Biomedical Research Centre, University of Southampton and University Hospital Southampton NHS Foundation Trust. Dr Raisi-Estabragh recognizes the National Institute for Health and Care Research Integrated Academic Training program (CL-2021-19-00), which supports her academic clinical lectureship post, and was also supported by British Heart Foundation Clinical Research Training Fellowship no. FS/17/81/33318. The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or decision to publish. The authors were not precluded from accessing data in the study, and they accept responsibility to submit for publication. Dr Petersen is as a consultant to Cardiovascular Imaging Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

References
-
- Quaresma M., Coleman M.P., Rachet B. 40-year trends in an index of survival for all cancers combined and survival adjusted for age and sex for each cancer in England and Wales, 1971-2011: a population-based study. Lancet. 2015;385(9974):1206–1218. - PubMed
-
- Cancer Treatment & Survivorship Facts & Figures 2022-2024. American Cancer Society. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-...
-
- Lyon A.R., López-Fernández T., Couch L.S., et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS) Eur Heart J. 2022;3:1–133. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
