

Adoption strategies of fertility-sparing surgery for early-stage cervical cancer patients based on clinicopathological characteristics: a large retrospective cohort study
- PMID: 39239473
- PMCID: PMC11375612
- DOI: 10.3389/fsurg.2024.1456376
Adoption strategies of fertility-sparing surgery for early-stage cervical cancer patients based on clinicopathological characteristics: a large retrospective cohort study
Abstract
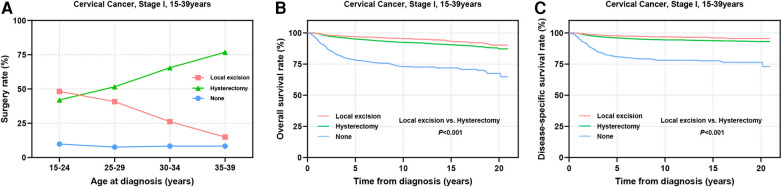
Background: The demand for fertility-sparing surgery (FSS) is increasing among patients with early-stage cervical cancer (CC). This study aimed to evaluate the feasibility of local excision as an alternative to hysterectomy in stage I CC patients aged 15-39 years-commonly referred to as adolescents and young adults (AYAs)-with varying clinicopathological characteristics.
Methods: Using the Surveillance, Epidemiology, and End Results (SEER) database, we identified patients diagnosed between 2000 and 2020. We examined treatment interventions across different age groups, degrees of histological types, tumor differentiation, and tumor stages. The effect of local excision vs. hysterectomy was assessed by comparing overall survival (OS) and disease-specific survival (DSS) rates.
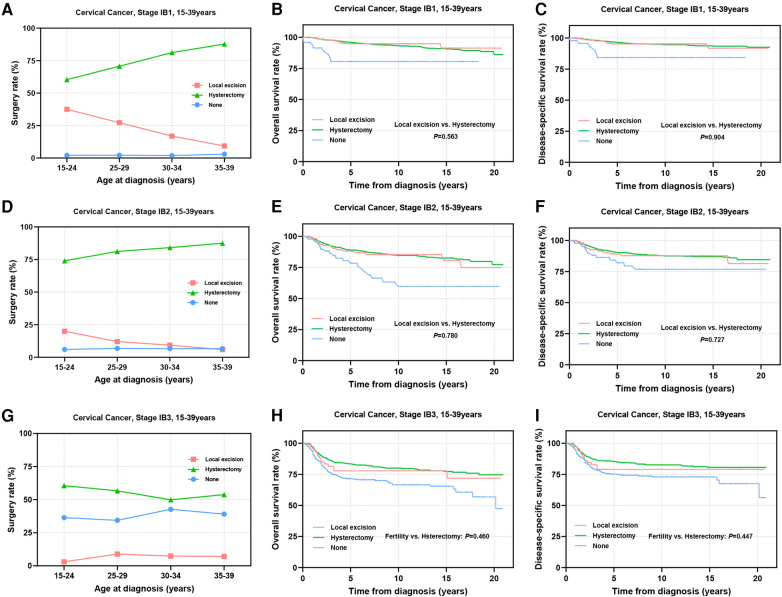
Results: A total of 10,629 stage I AYA cervical cancer patients were included in this study. Among these patients, 24.5% underwent local excision for fertility preservation, while 67.3% underwent radical hysterectomy. For patients with cervical squamous cell carcinoma (SCC), long-term outcomes favored local excision over hysterectomy, and a similar trend was observed in those with adenosquamous cell carcinoma (ASCC). However, the prognosis was comparable among patients with cervical adenocarcinoma (AC). In patients with well- and moderate- differentiated tumors, local excision demonstrated superior OS compared to hysterectomy. No significant differences in prognosis were found between the two surgical interventions for patients with poorly differentiated and undifferentiated tumors. In stage IA patients, local excision was considered a viable alternative to hysterectomy. In stage IB1-IB2, FSS yielded prognostic outcomes comparable to those of hysterectomy. Conversely, patients with stage IB3 exhibited significantly shorter 5-year OS and DSS following local excision than those who underwent hysterectomy.
Conclusion: In stage IA-IB2 (diameter ≤4 cm) AYA patients, local excision may serve as a viable option for fertility preservation. The histological type of SCC, AC, and ASCC, along with differentiation, should not serve as restrictive factors in determining fertility preservation strategies for these patients. Patients with early-stage, well- or moderately-differentiated SCC may benefit from local excision surgery, even when fertility preservation is not the primary objective.
Keywords: early-stage cervical cancer; fertility preservation; hysterectomy; local excision; prognosis.
© 2024 Ning, Gao, Kong, Wang, Tian, Chen, Yang, Lei and Cui.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- World Health Organization. International Agency for Research on Cancer (Iarc), Global Cancer Observatory (Gco). Available online at: https://Gco.Iarc.Fr (accessed April 18, 2024)
LinkOut - more resources
Full Text Sources
Research Materials