

Correlation between coronary calcification and cardiac structure in non-dialysis patients with chronic kidney disease
- PMID: 39239806
- PMCID: PMC11769669
- DOI: 10.1002/ehf2.15057
Correlation between coronary calcification and cardiac structure in non-dialysis patients with chronic kidney disease
Abstract
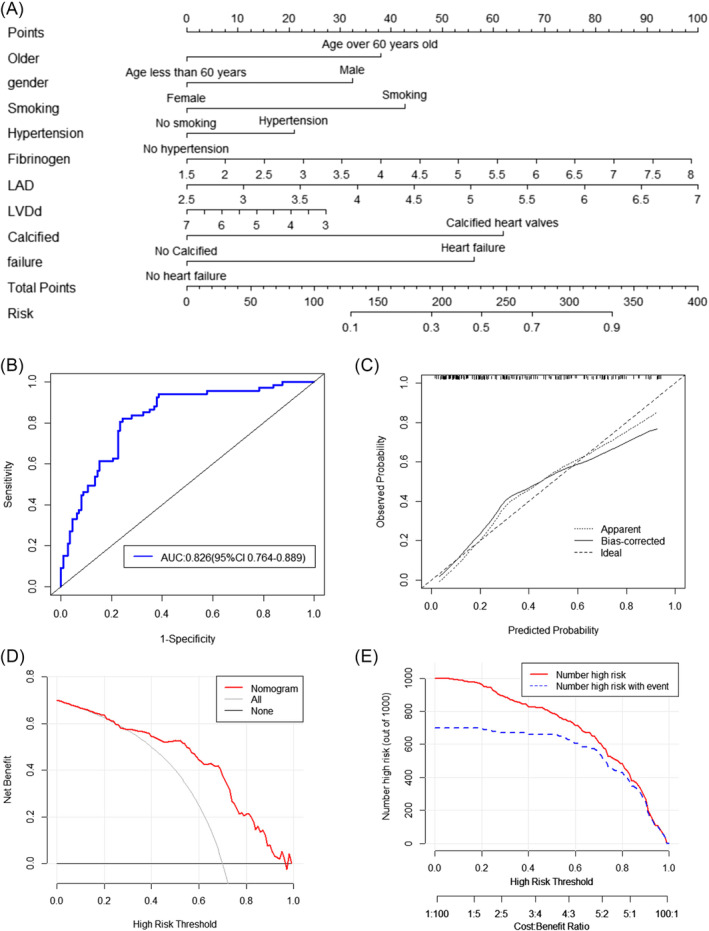
Aims: We aim to explore the correlation between coronary artery calcification (CAC) score (CACS) and cardiac structure and function in chronic kidney disease (CKD) patients, create a clinical prediction model for severe CAC associated with cardiac ultrasound indexes.
Methods and results: The study included 178 non-dialysis CKD patients who underwent CACS testing and collected general information, serological indices, cardiac ultrasound findings and follow-up on renal function, heart failure (HF) manifestations and re-hospitalization. The mean age of participants in the study cohort was 67.4 years; 59% were male, and 66.9% of patients had varying degrees of comorbid CAC. CKD patients with CACS > 100 were older, predominantly male and had a higher proportion of smoking, diabetes and hypertension (P < 0.05) compared with those with CACS = 0 and 0 < CACS ≤ 100, and had higher brain natriuretic peptide, serum magnesium and fibrinogen levels were also higher (P < 0.05). CACS was positively correlated with left atrial inner diameter (LAD), left ventricular end-diastolic inner diameter (LVDd), left ventricular volume at diastole (LVVd), output per beat (SV) and mitral orifice early diastolic blood flow velocity/early mitral annular diastolic myocardial motion velocity (E/e) (P < 0.05). We tested the associations between varying degrees of CAC and HF and heart valve calcification using multivariable-adjusted regression models. The risk of HF in patients with severe CAC was about 1.95 times higher than that in patients without coronary calcification, and the risk of heart valve calcification was 2.46 times higher than that in patients without coronary calcification. Heart valve calcification and HF diagnosis, LAD and LVDd are essential in predicting severe CAC. During a mean follow-up time of 18.26 ± 10.17 months, 65 (36.52%) patients had a composite renal endpoint event, of which 36 (20.22%) were admitted to renal replacement therapy. Patients with severe CAC had a higher risk of progression of renal function, re-admission due to cardiovascular and renal events and more pronounced symptoms of HF (P < 0.05).
Conclusions: There is a correlation between CACS and cardiac structure and function in non-dialysis CKD patients, which may mainly involve abnormalities in left ventricular structure and cardiac diastolic function. CAC may affect renal prognosis and quality of survival in CKD patients. Based on clinical information, HF, valvular calcification status and indicators related to left ventricular hypertrophy can identify people at risk for severe CAC.
Keywords: cardiovascular events; chronic kidney disease; clinical prediction models; coronary artery calcification.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures




References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
