

Lung-innervating nociceptor sensory neurons promote pneumonic sepsis during carbapenem-resistant Klebsiella pneumoniae lung infection
- PMID: 39241063
- PMCID: PMC11378917
- DOI: 10.1126/sciadv.adl6162
Lung-innervating nociceptor sensory neurons promote pneumonic sepsis during carbapenem-resistant Klebsiella pneumoniae lung infection
Abstract
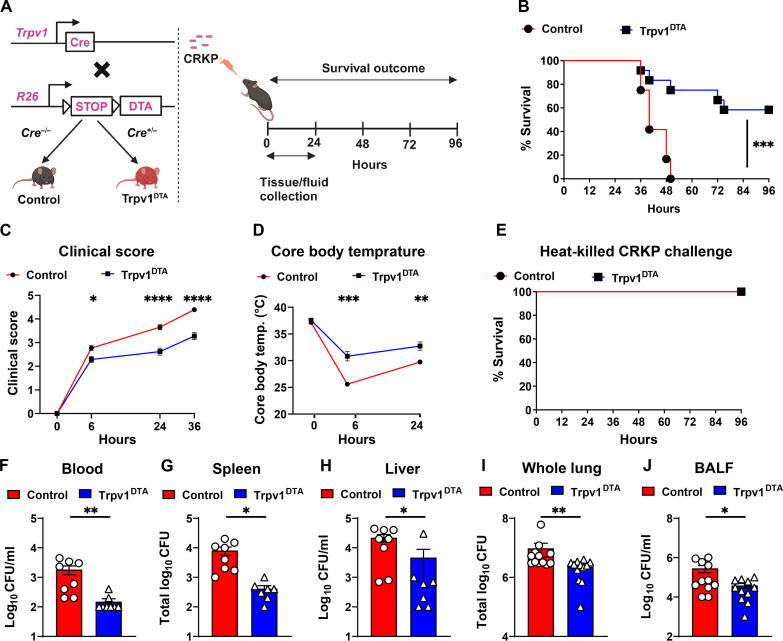
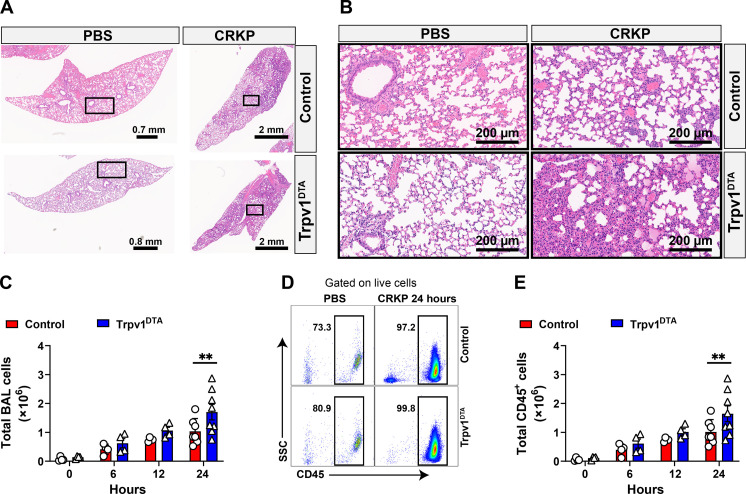
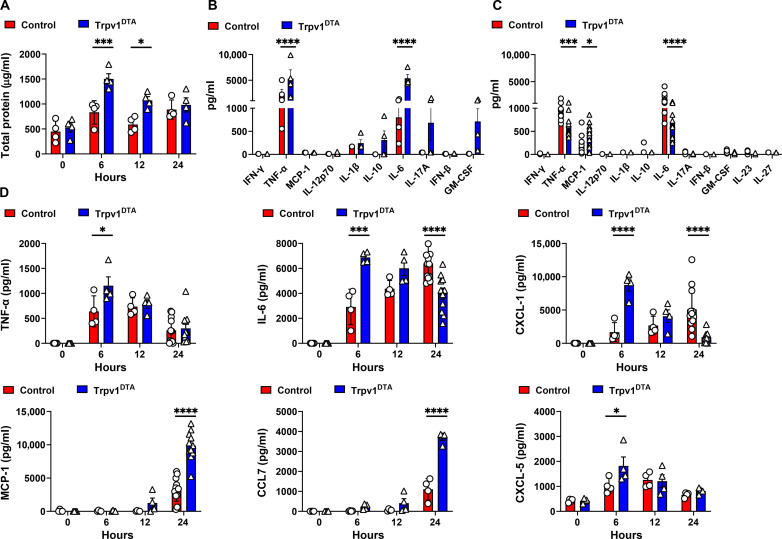
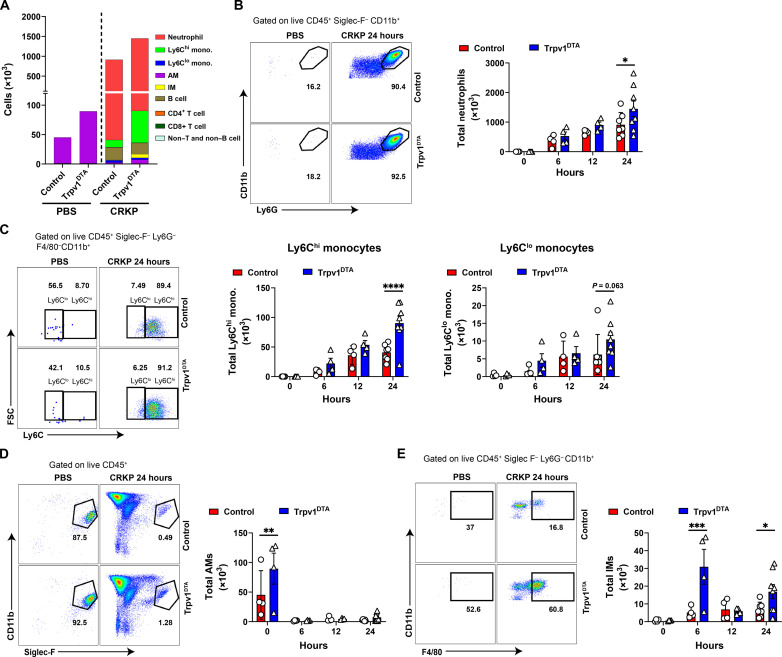
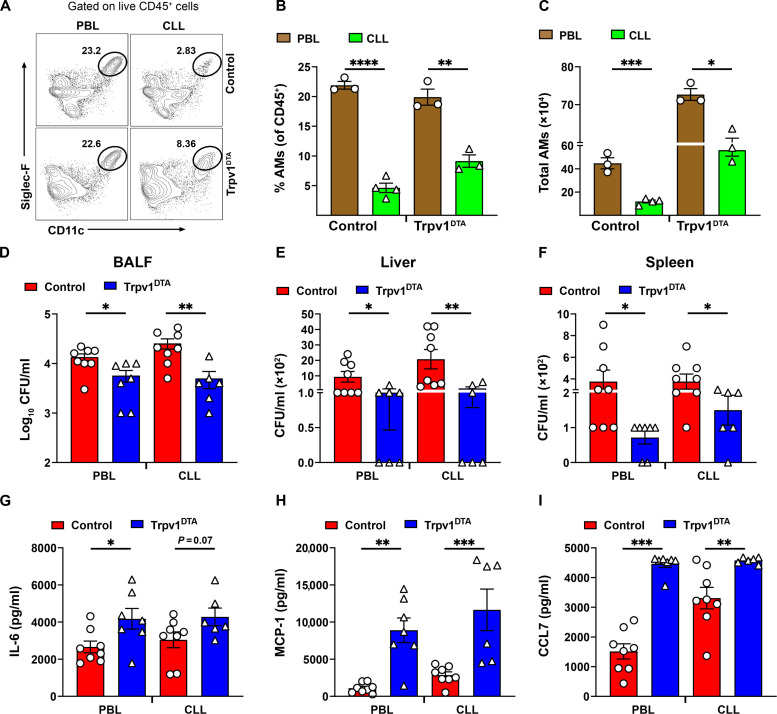
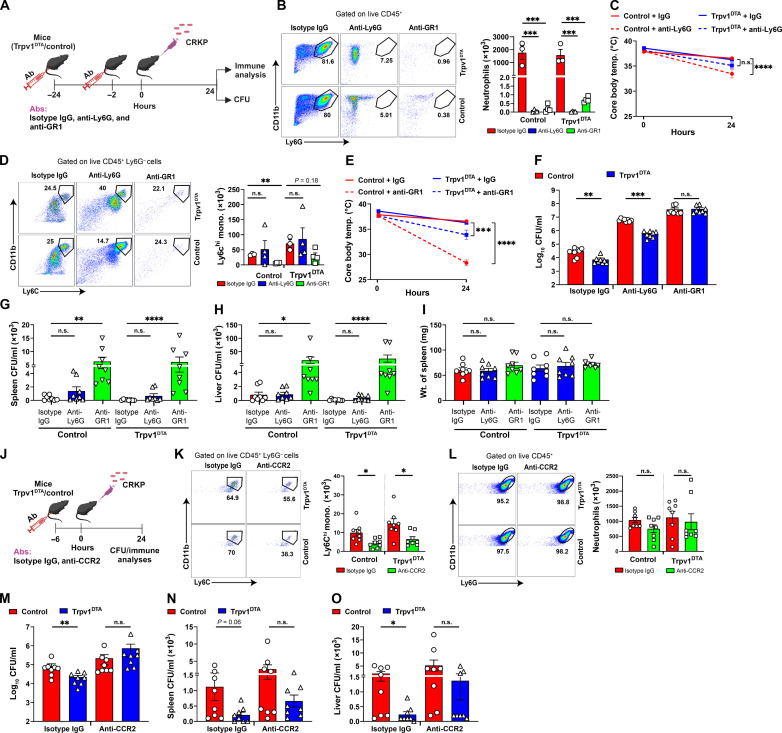
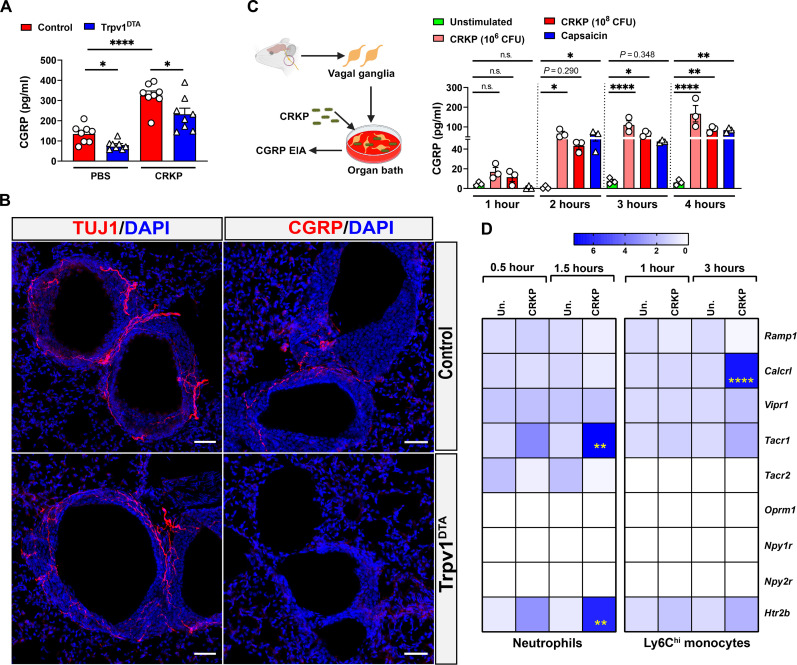
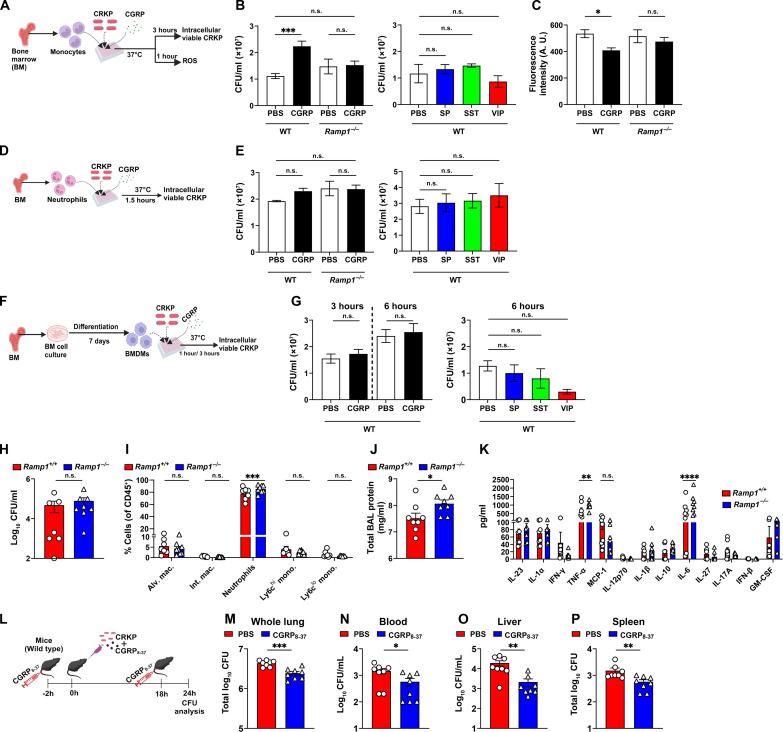
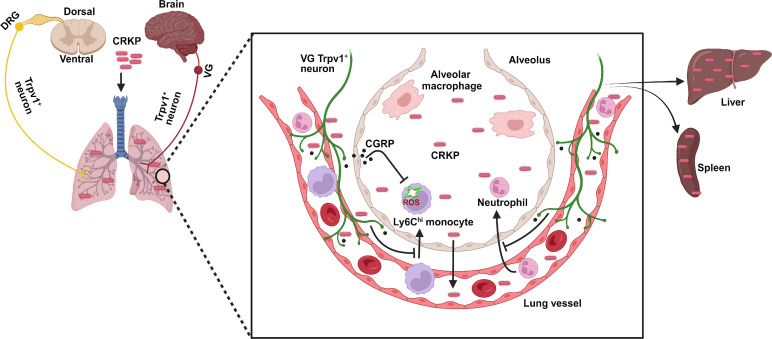
Carbapenem-resistant Klebsiella pneumoniae (CRKP) causes Gram-negative lung infections and fatal pneumonic sepsis for which limited therapeutic options are available. The lungs are densely innervated by nociceptor sensory neurons that mediate breathing, cough, and bronchoconstriction. The role of nociceptors in defense against Gram-negative lung pathogens is unknown. Here, we found that lung-innervating nociceptors promote CRKP pneumonia and pneumonic sepsis. Ablation of nociceptors in mice increased lung CRKP clearance, suppressed trans-alveolar dissemination of CRKP, and protected mice from hypothermia and death. Furthermore, ablation of nociceptors enhanced the recruitment of neutrophils and Ly6Chi monocytes and cytokine induction. Depletion of Ly6Chi monocytes, but not of neutrophils, abrogated lung and extrapulmonary CRKP clearance in ablated mice, suggesting that Ly6Chi monocytes are a critical cellular population to regulate pneumonic sepsis. Further, neuropeptide calcitonin gene-related peptide suppressed the induction of reactive oxygen species in Ly6Chi monocytes and their CRKP-killing abilities. Targeting nociceptor signaling could be a therapeutic approach for treating multidrug-resistant Gram-negative infection and pneumonic sepsis.
Figures
References
-
- Kang C. I., Song J. H., Kim S. H., Chung D. R., Peck K. R., Thamlikitkul V., Wang H., So T. M., Hsueh P. R., Yasin R. M., Carlos C. C., Van P. H., Perera J., Risk factors and pathogenic significance of bacteremic pneumonia in adult patients with community-acquired pneumococcal pneumonia. J. Infect. 66, 34–40 (2013). - PubMed
-
- Nair H., Simoes E. A., Rudan I., Gessner B. D., Azziz-Baumgartner E., Zhang J. S. F., Feikin D. R., Mackenzie G. A., Moiisi J. C., Roca A., Baggett H. C., Zaman S. M., Singleton R. J., Lucero M. G., Chandran A., Gentile A., Cohen C., Krishnan A., Bhutta Z. A., Arguedas A., Clara A. W., Andrade A. L., Ope M., Ruvinsky R. O., Hortal M., McCracken J. P., Madhi S. A., Bruce N., Qazi S. A., Morris S. S., El Arifeen S., Weber M. W., Scott J. A. G., Brooks W. A., Breiman R. F., Campbell H.; Severe Acute Lower Respiratory Infections Working Group , Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: A systematic analysis. Lancet 381, 1380–1390 (2013). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
