

Capivasertib and fulvestrant for patients with hormone receptor-positive advanced breast cancer: characterization, time course, and management of frequent adverse events from the phase III CAPItello-291 study
- PMID: 39241495
- PMCID: PMC11406080
- DOI: 10.1016/j.esmoop.2024.103697
Capivasertib and fulvestrant for patients with hormone receptor-positive advanced breast cancer: characterization, time course, and management of frequent adverse events from the phase III CAPItello-291 study
Abstract
Background: Capivasertib is a potent, selective pan-AKT inhibitor. In CAPItello-291, the addition of capivasertib to fulvestrant resulted in a statistically significant (P < 0.001) improvement in progression-free survival over fulvestrant monotherapy in patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer and disease progression on or after aromatase inhibitor-based therapy. Characterization of the capivasertib-fulvestrant adverse event (AE) profile as managed in CAPItello-291 can inform future management guidance and optimize clinical benefit.
Patients and methods: Seven hundred and eight patients were randomized 1 : 1 to capivasertib (400 mg twice daily; 4 days on, 3 days off) or placebo, plus fulvestrant, on a 4-week cycle. Dose reductions/interruptions for capivasertib/placebo were permitted (up to two dose reductions). Safety analyses included exposure, AE, and clinical laboratory data and were conducted in patients who received at least one dose of capivasertib, fulvestrant, or placebo. Frequent AEs associated with phosphoinositide 3-kinase (PI3K)/protein kinase (AKT) pathway inhibition (diarrhea, rash, hyperglycemia) were characterized using group terms. AEs were summarized using descriptive statistics; time-to-event analyses were conducted.
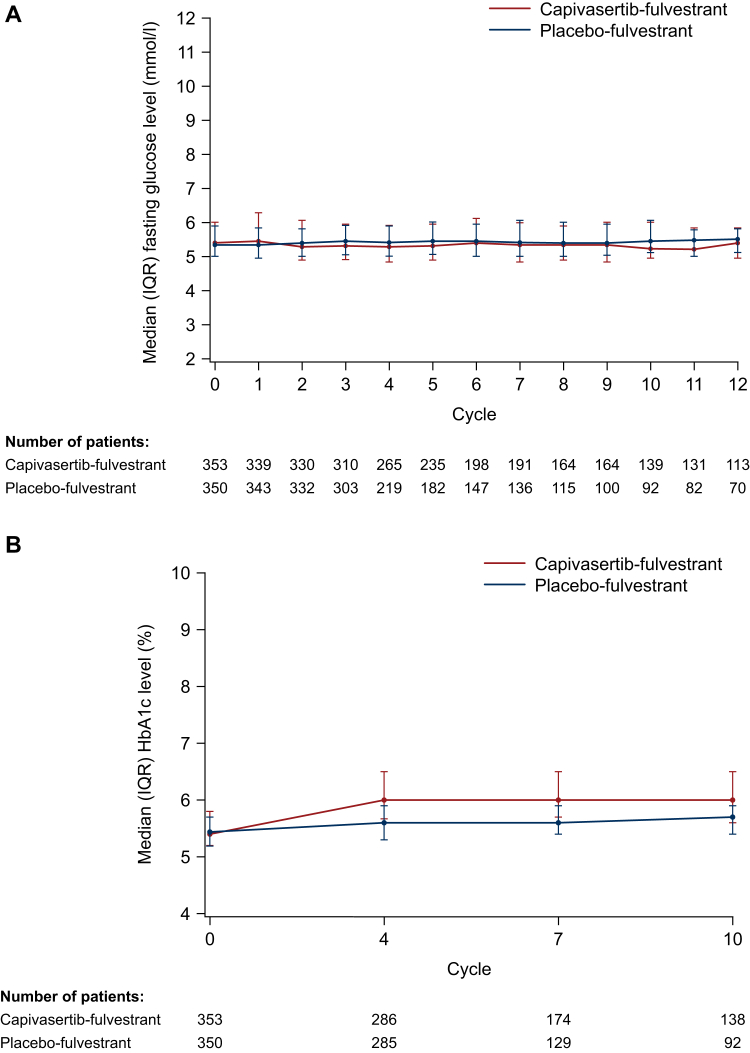
Results: Safety analyses included 705 patients: capivasertib-fulvestrant (n = 355) and placebo-fulvestrant (n = 350). Frequent any-grade AEs with capivasertib-fulvestrant were diarrhea (72.4%), rash (38.0%), and nausea (34.6%); frequent grade ≥3 AEs were rash (12.1%), diarrhea (9.3%), and hyperglycemia (2.3%). Diarrhea, rash, and hyperglycemia occurred shortly after starting capivasertib-fulvestrant [median days to onset (interquartile range) of any grade: 8 (2-22), 12 (10-15), and 15 (1-51), respectively], and were managed with supportive medications, dose reductions, interruptions, and/or discontinuation. Discontinuation rates were 2.0%, 4.5%, and 0.3%, respectively. Overall, 13.0% discontinued capivasertib due to AEs.
Conclusions: Frequent AEs associated with PI3K/AKT pathway inhibition occurred early and were manageable. The low rate of treatment discontinuations suggests that, when appropriately managed, these AEs do not pose a challenge to clinical benefit.
Keywords: advanced breast cancer; capivasertib; diarrhea; hyperglycemia; rash; safety.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer (Version 2.2024) © National Comprehensive Cancer Network, Inc. 2024 https://www.nccn.org/guidelines/category_1 All rights reserved. Available at. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way at the end as this is a requirement on NCCN and the reference was approved by them with these additions.
-
- Gennari A., André F., Barrios C.H., et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–1495. - PubMed
-
- Millis S.Z., Ikeda S., Reddy S., et al. Landscape of phosphatidylinositol-3-kinase pathway alterations across 19 784 diverse solid tumors. JAMA Oncol. 2016;2(12):1565–1573. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
