

Short-term outcomes of Transrectal Natural Orifice Specimen extraction compared with conventional minimally invasive surgery for selected patients with colorectal cancer: a propensity score matching analysis and literature review
- PMID: 39242550
- PMCID: PMC11380319
- DOI: 10.1186/s12957-024-03513-3
Short-term outcomes of Transrectal Natural Orifice Specimen extraction compared with conventional minimally invasive surgery for selected patients with colorectal cancer: a propensity score matching analysis and literature review
Abstract
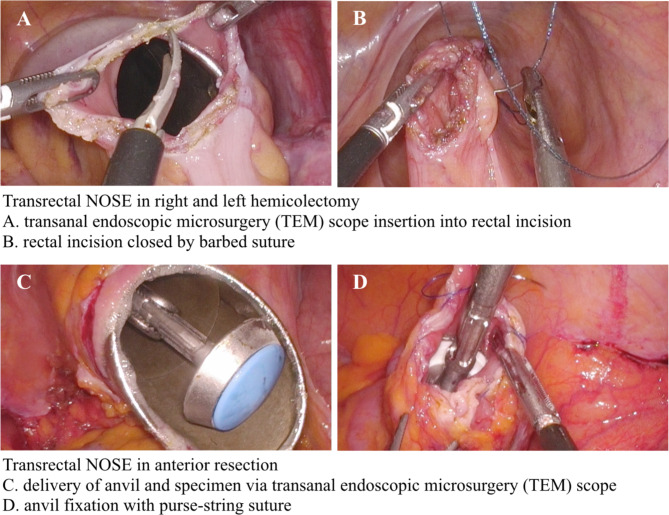
Purpose: Conventional minimally invasive surgery requires mini-laparotomy to extract the pathological specimen. However, by using a natural orifice as the delivery route, natural orifice specimen extraction (NOSE) surgery avoids the need for a large incision. This study analyzed the short-term outcome of NOSE compared with conventional mini-laparotomy (CL) for colorectal cancer surgery.
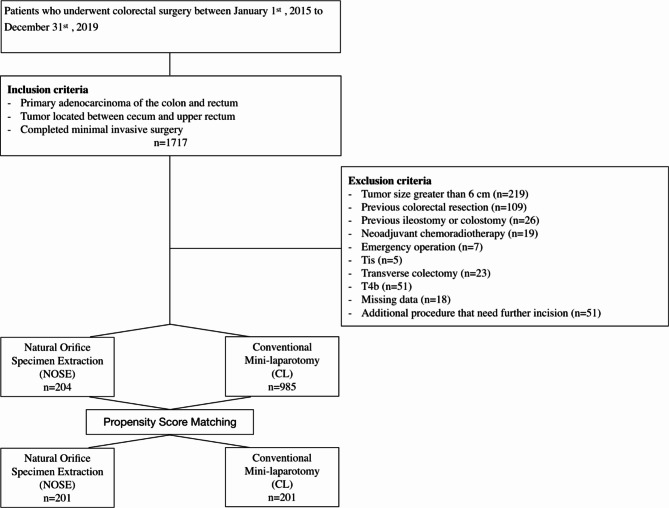
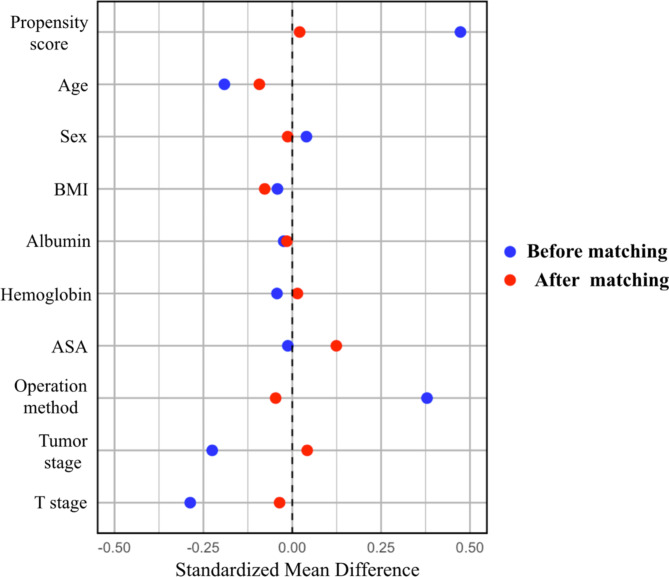
Methods: We conducted a retrospective analysis of 1,189 patients who underwent surgery for primary colorectal cancer between the cecum and upper rectum. Propensity score analyses were applied to the NOSE and CL groups in a 1:1 matched cohort.
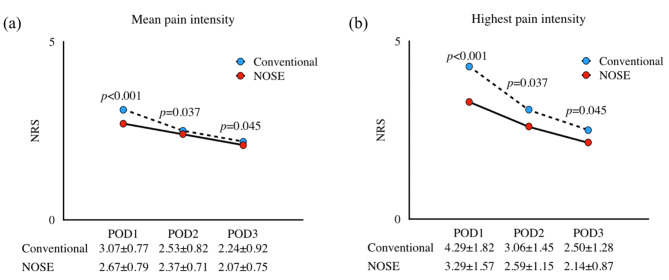
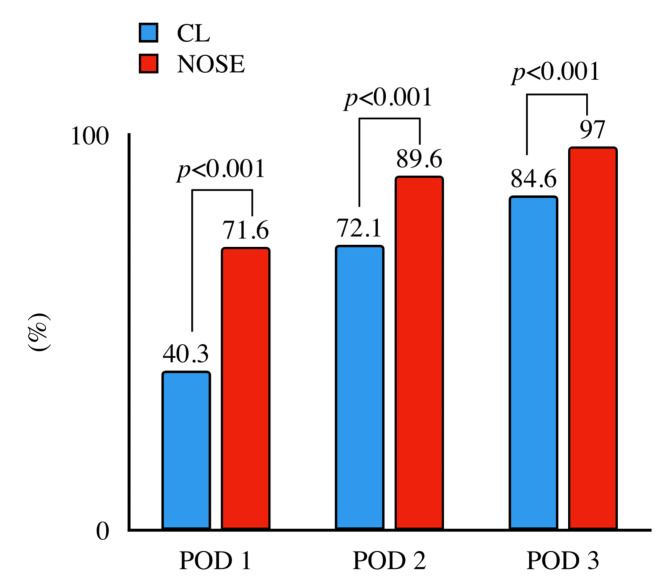
Results: After propensity score matching, each group included 201 patients. The NOSE group and CL group did not differ significantly in terms of baseline characteristics. Postoperative morbidity and mortality rates were comparable. Compared with the CL group, the NOSE group experienced a shorter time to first flatus (1.6 ± 0.8 vs. 2.0 ± 1.2 days, p < 0.001), first stool (2.7 ± 1.5 vs. 4.1 ± 1.9, p < 0.001), liquid diet (2.3 ± 1.3 vs. 3.6 ± 1.8 days, p < 0.001), soft diet (3.9 ± 2.0 vs. 5.2 ± 1.9 days, p < 0.001) and a shorter hospital stay (5.1 ± 3.5 vs. 7.4 ± 4.8 days, p < 0.001). The NOSE group exhibited lower mean pain intensity and lower highest pain intensity on postoperative days 1, 2, and 3.
Conclusion: NOSE has several advantages over conventional mini-laparotomy following minimally invasive surgery for colon cancer. These advantages include reduced time to oral intake, shorter hospital stays, and less postoperative pain. NOSE can be adopted and applied to highly selective patients without additional risk of short-term complications.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
The authors declare no competing interests.
Figures
Similar articles
-
Minimally invasive right colectomy with transrectal natural orifice extraction: could this be the next step forward?Tech Coloproctol. 2020 Nov;24(11):1197-1205. doi: 10.1007/s10151-020-02282-x. Epub 2020 Jul 6. Tech Coloproctol. 2020. PMID: 32632708 Free PMC article.
-
Propensity score-matched comparison between totally laparoscopic right hemicolectomy with transcolonic natural orifice specimen extraction and conventional laparoscopic surgery with mini-laparotomy in the treatment of ascending colon cancer (with video).Gastrointest Endosc. 2021 Sep;94(3):642-650. doi: 10.1016/j.gie.2021.03.028. Epub 2021 Mar 31. Gastrointest Endosc. 2021. PMID: 33798538
-
Natural orifice versus conventional mini-laparotomy for specimen extraction after reduced-port laparoscopic surgery for colorectal cancer: propensity score-matched comparative study.Surg Endosc. 2022 Jan;36(1):155-166. doi: 10.1007/s00464-020-08250-8. Epub 2021 Feb 2. Surg Endosc. 2022. PMID: 33532930
-
Natural Orifice Extraction Techniques (Natural Orifice Specimen Extraction and Natural Orifice Transluminal Endoscopic Surgery) for Left-Sided Colorectal Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Laparoendosc Adv Surg Tech A. 2025 May;35(5):379-387. doi: 10.1089/lap.2025.0003. Epub 2025 Mar 28. J Laparoendosc Adv Surg Tech A. 2025. PMID: 40152871
-
Comparative analysis of safety and effectiveness between natural orifice specimen extraction and conventional transabdominal specimen extraction in robot-assisted colorectal cancer resection through systematic review and meta-analysis.J Robot Surg. 2024 Oct 3;18(1):360. doi: 10.1007/s11701-024-02106-2. J Robot Surg. 2024. PMID: 39361096
Cited by
-
Mini-laparotomy versus transrectal natural orifice specimen extraction for minimally invasive colorectal cancer surgery: study protocol for a randomized controlled trial (MINITR-NOSE trial, TCAR2514 protocol).Trials. 2025 Aug 25;26(1):304. doi: 10.1186/s13063-025-09039-7. Trials. 2025. PMID: 40855494
References
-
- Nelson H, Sargent DJ, Wieand HS, et al. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med May. 2004;13(20):2050–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
