

Maternal Streptococcus agalactiae colonization in Europe: data from the multi-center DEVANI study
- PMID: 39244714
- PMCID: PMC11825526
- DOI: 10.1007/s15010-024-02380-0
Maternal Streptococcus agalactiae colonization in Europe: data from the multi-center DEVANI study
Abstract
Introduction: Despite national guidelines and use of intrapartum antibiotic prophylaxis (IAP), Streptococcus agalactiae (group B streptococci (GBS)) is still a leading cause of morbidity and mortality in newborns in Europe and the United States. The European DEVANI (Design of a Vaccine Against Neonatal Infections) program assessed the neonatal GBS infection burden in Europe, the clinical characteristics of colonized women and microbiological data of GBS strains in colonized women and their infants with early-onset disease (EOD).
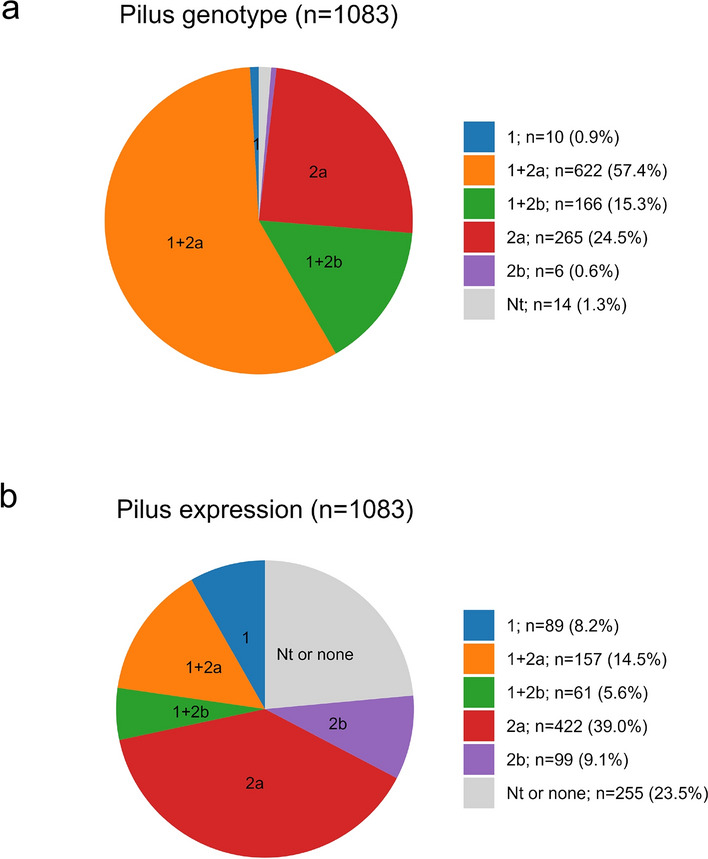
Methods: Overall, 1083 pregnant women with a GBS-positive culture result from eight European countries were included in the study. Clinical obstetrical information was collected by a standardized questionnaire. GBS strains were characterized by serological and molecular methods.
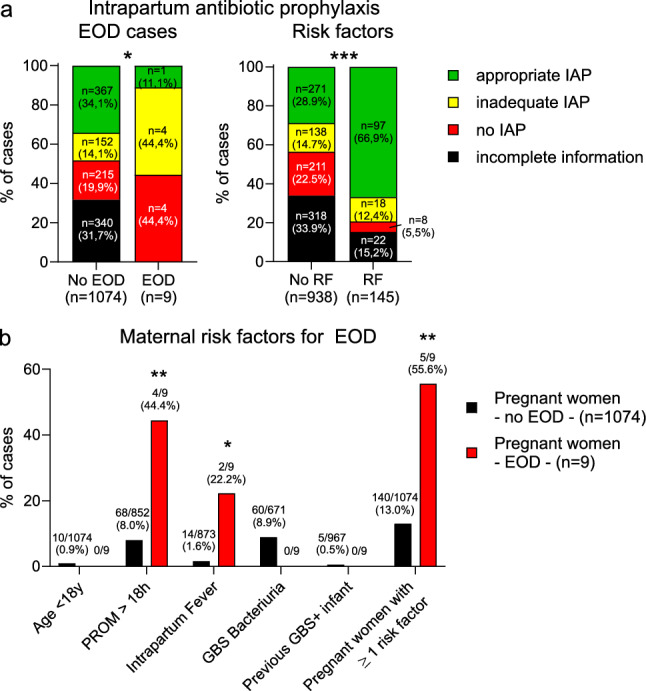
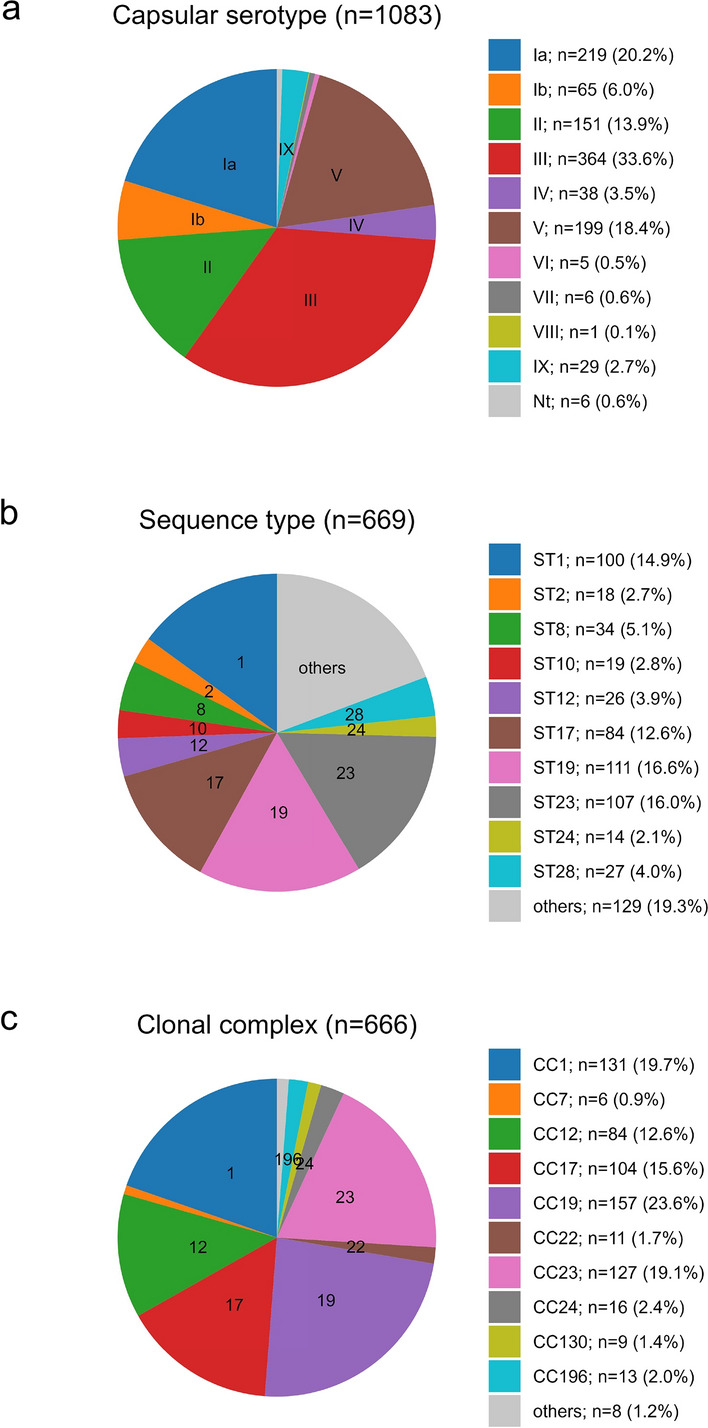
Results: Among GBS carriers included in this study after testing positive for GBS by vaginal or recto-vaginal sampling, 13.4% had at least one additional obstetrical risk factor for EOD. The five most common capsular types (i.e., Ia, Ib, II, III and V) comprised ~ 93% of GBS carried. Of the colonized women, 77.8% received any IAP, and in 49.5% the IAP was considered appropriate. In our cohort, nine neonates presented with GBS early-onset disease (EOD) with significant regional heterogeneity.
Conclusions: Screening methods and IAP rates need to be harmonized across Europe in order to reduce the rates of EOD. The epidemiological data from eight different European countries provides important information for the development of a successful GBS vaccine.
Keywords: Streptococcus agalactiae; Early-onset disease; GBS vaccine; Group B streptococcus; Intrapartum prophylaxis; Maternal colonization; Neonatal sepsis; Vertical transmission.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Financial interests: Margarit I, Maione D and Rinaudo D are employees of the GSK group of companies and hold shares in the GSK group of companies. Margarit I, Maione D and Rinaudo D are listed as inventor on patents owned by the GSK group of companies. Uffe B. Skov Sørensen and Mogens Kilian received personal consultancy fees from Suzhou VACMICRO Biotech Co., Ltd. Non-financial interests: Markus Hufnagel has been invited by Novartis to an advisory board meeting on juvenile idiopathic arthritis. Pierrette Melin has provided one scientific consultation for GSK vaccines. All other authors have no financial or non-financial interests to disclose. Ethical approval: The study was approved by local ethics committees of each participating institution, and informed consent for study participation has been obtained from the legal caregivers. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Figures
References
-
- Melin P, Efstratiou A. Group B streptococcal epidemiology and vaccine needs in developed countries. Vaccine. 2013;31:D31-42. 10.1016/j.vaccine.2013.05.012. - PubMed
-
- Schrag SJ, Zywicki S, Farley MM, Reingold AL, Harrison LH, Lefkowitz LB, Hadler JL, Danila R, Cieslak PR, Schuchat A. Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. N Engl J Med. 2000;342:15–20. 10.1056/NEJM200001063420103. - PubMed
-
- Edmond KM, Kortsalioudaki C, Scott S, Schrag SJ, Zaidi AKM, Cousens S, Heath PT. Group B streptococcal disease in infants aged younger than 3 months: systematic review and meta-analysis. Lancet. 2012;379:547–56. 10.1016/S0140-6736(11)61651-6. - PubMed
-
- Puopolo KM, Lynfield R, Cummings JJ, Hand I, Adams-Chapman I, Poindexter B, Stewart DL, Aucott SW, Goldsmith JP, Mowitz M, Watterberg K, Maldonado YA, Zaoutis TE, Banerjee R, Barnett ED, Campbell JD, Gerber JS, Kourtis AP, Munoz FM, Nolt D, Nyquist AC, O’Leary ST, Sawyer MH, Steinbach WJ, Zangwill K, Committee on fetus and newborn, Committee on infectious diseases. Management of infants at risk for group B Streptococcal disease. Pediatrics. 2019;144:e20191881. 10.1542/peds.2019-1881. - PubMed
-
- Lohrmann F, Hufnagel M, Kunze M, Afshar B, Creti R, Detcheva A, Kozakova J, Rodriguez-Granger J, Sørensen UBS, Margarit I, Maione D, Rinaudo D, Orefici G, Telford J, de la Rosa FM, Kilian M, Efstratiou A, Berner R, Melin P. Neonatal invasive disease caused by Streptococcus agalactiae in Europe: the DEVANI multi-center study. Infection. 2023;51:981–91. 10.1007/s15010-022-01965-x. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
