

Non-invasive optoacoustic imaging of glycogen-storage and muscle degeneration in late-onset Pompe disease
- PMID: 39245687
- PMCID: PMC11381542
- DOI: 10.1038/s41467-024-52143-6
Non-invasive optoacoustic imaging of glycogen-storage and muscle degeneration in late-onset Pompe disease
Abstract
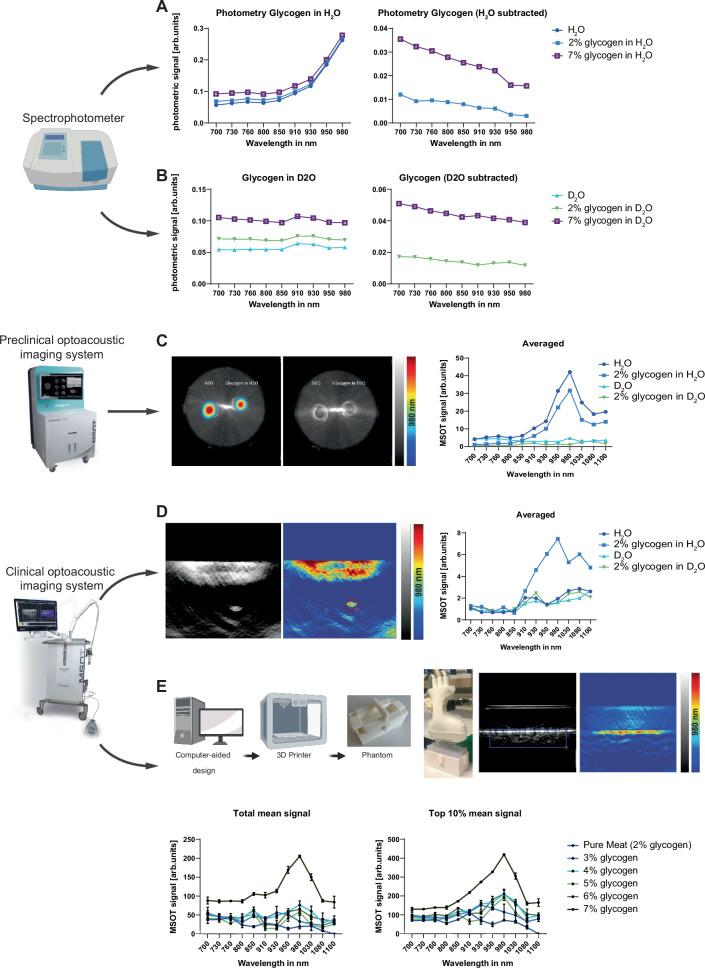
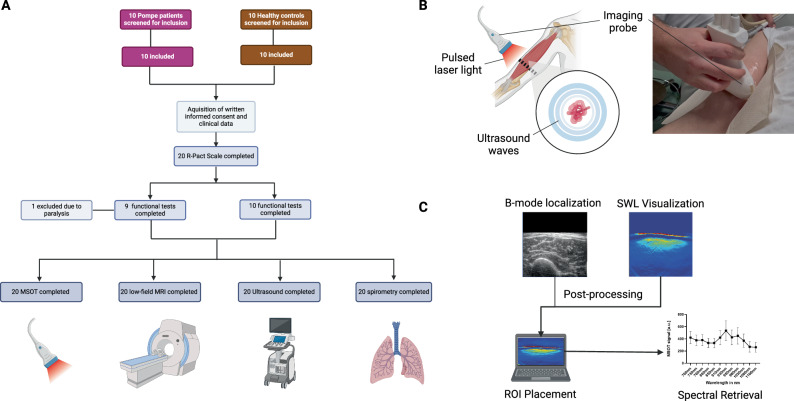
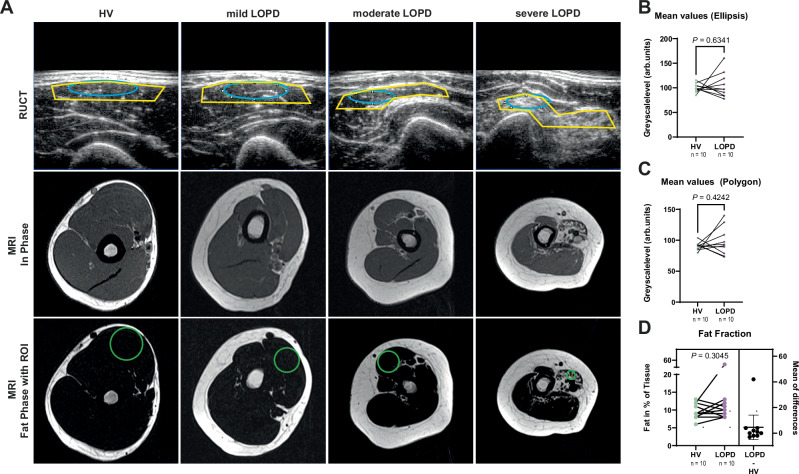
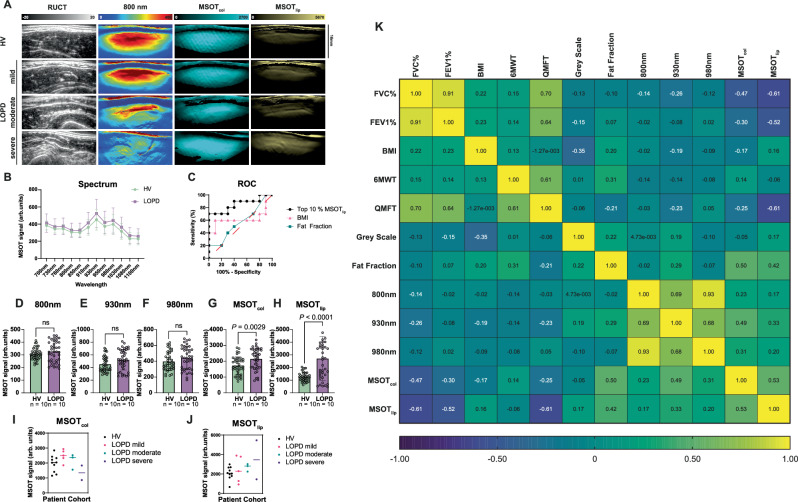
Pompe disease (PD) is a rare autosomal recessive glycogen storage disorder that causes proximal muscle weakness and loss of respiratory function. While enzyme replacement therapy (ERT) is the only effective treatment, biomarkers for disease monitoring are scarce. Following ex vivo biomarker validation in phantom studies, we apply multispectral optoacoustic tomography (MSOT), a laser- and ultrasound-based non-invasive imaging approach, in a clinical trial (NCT05083806) to image the biceps muscles of 10 late-onset PD (LOPD) patients and 10 matched healthy controls. MSOT is compared with muscle magnetic resonance imaging (MRI), ultrasound, spirometry, muscle testing and quality of life scores. Next, results are validated in an independent LOPD patient cohort from a second clinical site. Our study demonstrates that MSOT enables imaging of subcellular disease pathology with increases in glycogen/water, collagen and lipid signals, providing higher sensitivity in detecting muscle degeneration than current methods. This translational approach suggests implementation in the complex care of these rare disease patients.
© 2024. The Author(s).
Conflict of interest statement
A.P.R. and F.K. are co-inventors together with iThera Medical GmbH, Germany, on an EU patent application (EP 19 163 304.9) relating to a device and a method for analyzing optoacoustic data, an optoacoustic system and a computer program. F.K. is a member of the advisory board of iThera Medical GmbH, Munich, Germany. A.P.R. and F.K. received travel support from iThera Medical GmbH, Germany. A.P.R., A.L.W., and F.K. report travel support from Sanofi Aventis, Germany. A.P.R. and F.K. report lecture fees from Sanofi Genzyme. F.K. reports lecture fees from Siemens Healthcare GmbH. The other authors declare no competing interests.
Figures
References
-
- Pompe, J. C. Over idiopathische hypertrophie van het hart. Ned. Tijdschr. Geneeskd.76, 304–311 (1932).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
