

Traumatic encephalocele in the nasal cavity after 6 years of trauma: a case report
- PMID: 39245767
- PMCID: PMC11382516
- DOI: 10.1186/s13256-024-04735-5
Traumatic encephalocele in the nasal cavity after 6 years of trauma: a case report
Abstract
Background: Encephalocele refers to protrusion of the meninges and brain tissue through a skull bone defect. It results from congenital, traumatic, neoplastic, or spontaneous reasons. Traumatic encephalocele occurs because of the posttraumatic fracture of the skull bone or iatrogenic causes. The manifestations vary a lot, such as rhinorrhea, seizures, headaches, and focal neurological deficits.
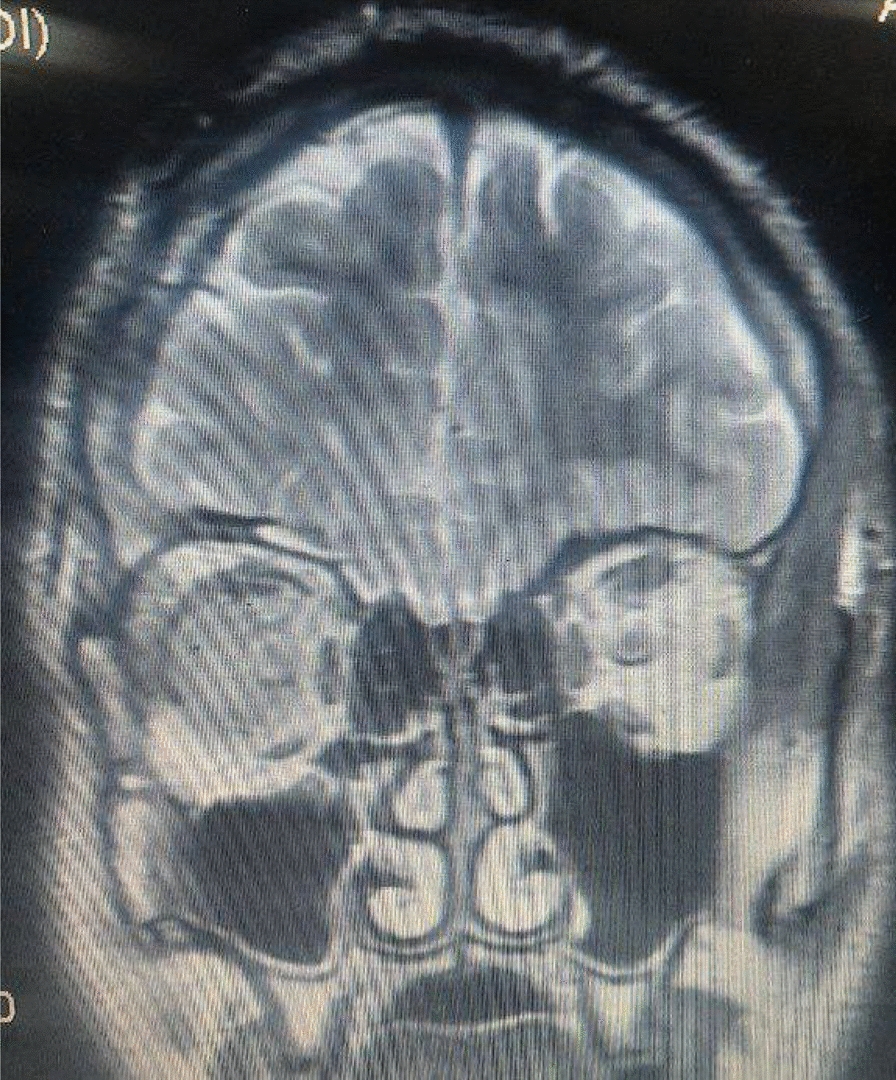
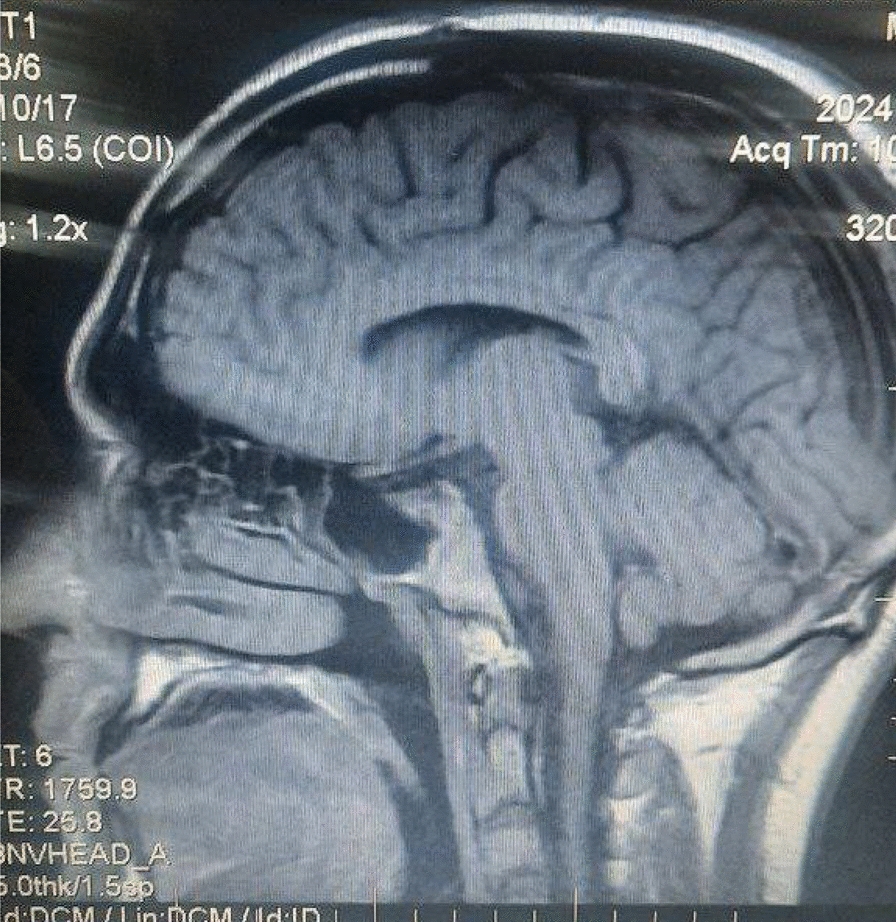
Case presentation: A 20-year-old Syrian male presented to our department with the complaint of clear cerebrospinal fluid drainage from his right nostril, which started 6 years ago after a head trauma, moderate headache, and episodes of tonic-clonic seizures without any response to medical treatment. Then, 2 months ago, the patient had meningoencephalitis, so he was admitted to the intensive care unit and treated for a month until he was cured. The patient underwent radiological investigations, which showed that he had a base fracture with an encephalocele in the nasal cavity. The brain tissues with the meninges herniated through the skull base fracture with a significant expansion of the subarachnoid spaces in the right hemisphere. He was advised to undergo surgical repair at that time, but he refused the surgery. During this visit, surgery was indicated. The surgery was done by a specialist who returned the herniated brain tissues to their normal location, repaired the meninges, and reconstructed the skull base with bone cement and bio-glue. The patient's recovery after the surgery was uneventful.
Conclusion: Traumatic encephalocele is a rare and unexpected complication of trauma, but we should keep it in mind when the patient comes with head trauma because of its life-threatening consequences. This complication can happen after years of trauma if the patient refuses treatment, therefore, we must educate patients about the dangerous results of neglecting cerebrospinal fluid leakage and skull fractures.
Keywords: Case report; Cerebrospinal fluid leakage; Fronto-ethmoidal bone; Meningitis; Seizures; Traumatic encephalocele.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- David DJ. Cephaloceles: classification, pathology, and management–a review. J Craniofac Surg. 1993;4(4):192–202. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
