

A systematic review and network meta-analysis of psychological, psychosocial, pharmacological, physical and combined treatments for adults with a new episode of depression
- PMID: 39246718
- PMCID: PMC11377144
- DOI: 10.1016/j.eclinm.2024.102780
A systematic review and network meta-analysis of psychological, psychosocial, pharmacological, physical and combined treatments for adults with a new episode of depression
Abstract
Background: Various effective treatments for depression exist. We aimed to identify the most effective first-line treatments for new episodes of less and more severe depression (defined by depression scale cut-off scores), to update NICE guidance on the management of Depression in Adults in England.
Methods: Systematic review and network meta-analysis of randomised controlled trials (RCTs) published up to June 2020 (PROSPERO registration number CRD42019151328). We analysed interventions by class and individually. The primary efficacy outcome was depressive symptom change (expressed as standardised mean difference [SMD]). The review for this outcome was updated in November 2023.
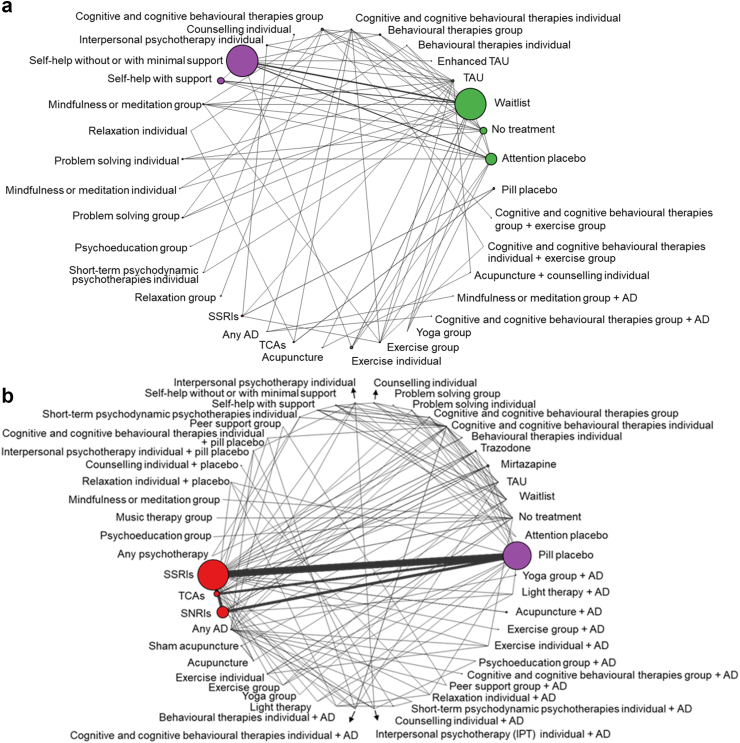
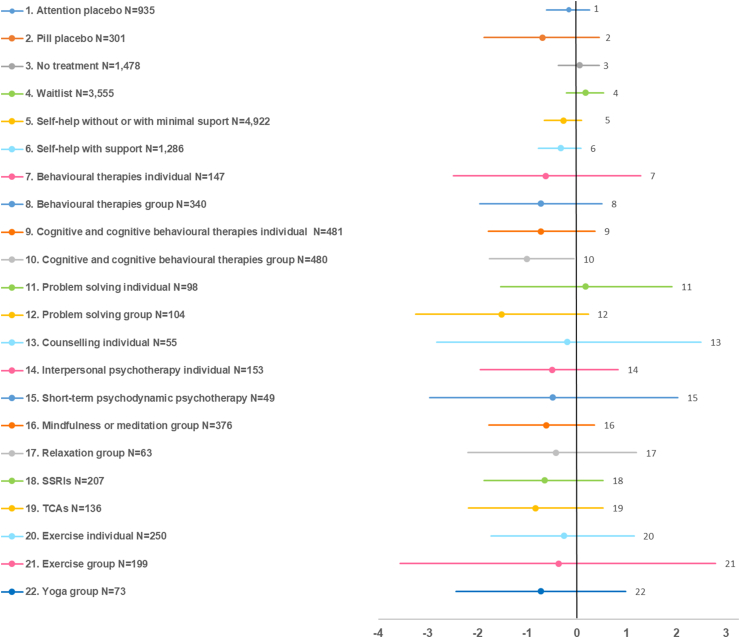
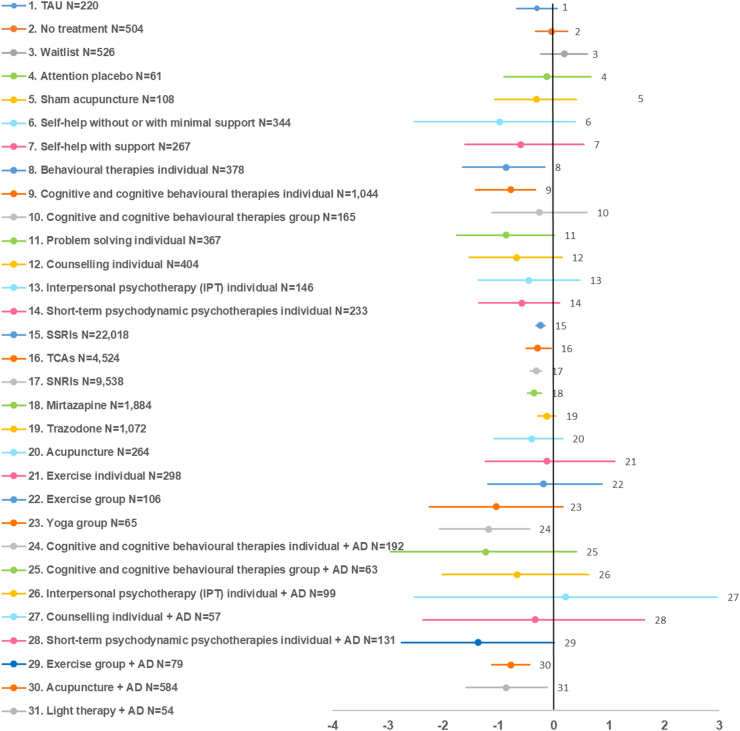
Findings: We included 676 RCTs, 105,477 participants and 63 treatment classes. For less severe depression, group cognitive/cognitive behavioural therapy (CT/CBT) class was efficacious versus treatment as usual [TAU], the reference treatment for this population [SMD -1.01 (95% Credible Interval [CrI] -1.76; -0.06)]. For more severe depression, efficacious classes versus pill placebo (reference treatment for this population) included combined individual CT/CBT with antidepressants [-1.18 (-2.07; -0.44)], individual behavioural therapies [-0.86 (-1.65; -0.16)], combined light therapy with antidepressants [-0.86 (-1.59; -0.12)], combined acupuncture with antidepressants [-0.78 (-1.12; -0.44)], individual CT/CBT [-0.78 (-1.42; -0.33)], mirtazapine [-0.35 (-0.48; -0.22)], serotonin and norepinephrine reuptake inhibitors [-0.32 (-0.43; -0.22)], tricyclic antidepressants [-0.29 (-0.50; -0.05)], and selective serotonin reuptake inhibitors [-0.24 (-0.32; -0.16)]. Additional treatments showed evidence of efficacy at the intervention level. Evidence for less and more severe depression was of low and low-to-moderate quality, respectively. In the 2023 update, group yoga and self-help without support emerged as efficacious for less severe depression. For more severe depression, combined group exercise with antidepressants emerged as efficacious, whereas combined light therapy with antidepressants failed to remain efficacious.
Interpretation: Group CT/CBT (and possibly group yoga and self-help) appears efficacious in less severe depression, whereas antidepressants do not show evidence of effect. Combined antidepressants with individual CT/CBT, acupuncture and, possibly, group exercise, individual psychological therapies (behavioural therapies, CT/CBT) alone, and antidepressants alone appear efficacious in more severe depression. Quality of evidence, cost-effectiveness, applicability and implementation issues also need to be considered when formulating clinical practice recommendations.
Funding: National Institute for Health and Care Excellence.
Keywords: Antidepressants; Clinical guidelines; Depression; Network meta-analysis; Physical interventions; Psychological interventions.
© 2024 The Author(s).
Conflict of interest statement
HE, KJMOD, IM, OMV, SA, SS and SP received support from NICE for the submitted work. CHD, DMC, HP, NJW, EK, and SD received support from the NICE Guidelines TSU for the submitted work. EW, NK and NN declared the following interests based on NICE's policy on conflicts of interests: https://www.nice.org.uk/guidance/ng222/documents/register-of-interests. The authors report no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- McCrone P., Dhanasiri S., Patel A., Knapp M., Lawton-Smith S. King's Fund; London: 2008. Paying the price. The cost of mental health care in England to 2026.
-
- Cuijpers P., Dekker J., Hollon S.D., Andersson G. Adding psychotherapy to pharmacotherapy in the treatment of depressive disorders in adults: a meta-analysis. J Clin Psychiatry. 2009;70(9):1219–1229. - PubMed
-
- Cuijpers P., van Straten A., Andersson G., van Oppen P. Psychotherapy for depression in adults: a meta-analysis of comparative outcome studies. J Consult Clin Psychol. 2008;76(6):909–922. - PubMed
LinkOut - more resources
Full Text Sources
