

Monoclonal antibodies against SARS-CoV-2 to prevent COVID-19 worsening in a large multicenter cohort
- PMID: 39247344
- PMCID: PMC11378919
- DOI: 10.1016/j.heliyon.2024.e36102
Monoclonal antibodies against SARS-CoV-2 to prevent COVID-19 worsening in a large multicenter cohort
Abstract
Objective: Monoclonal antibodies (mAbs) against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) reduced Coronavirus Disease 2019 (COVID-19) hospitalizations in people at risk of clinical worsening. Real-world descriptions are limited.
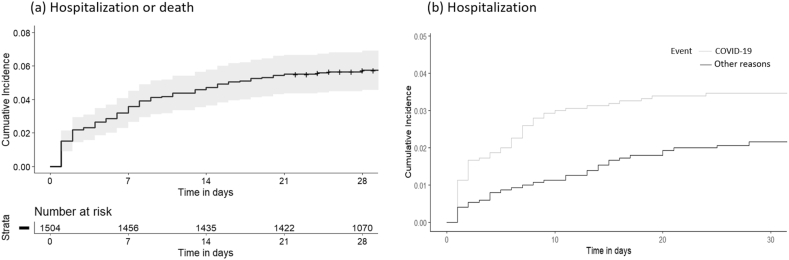
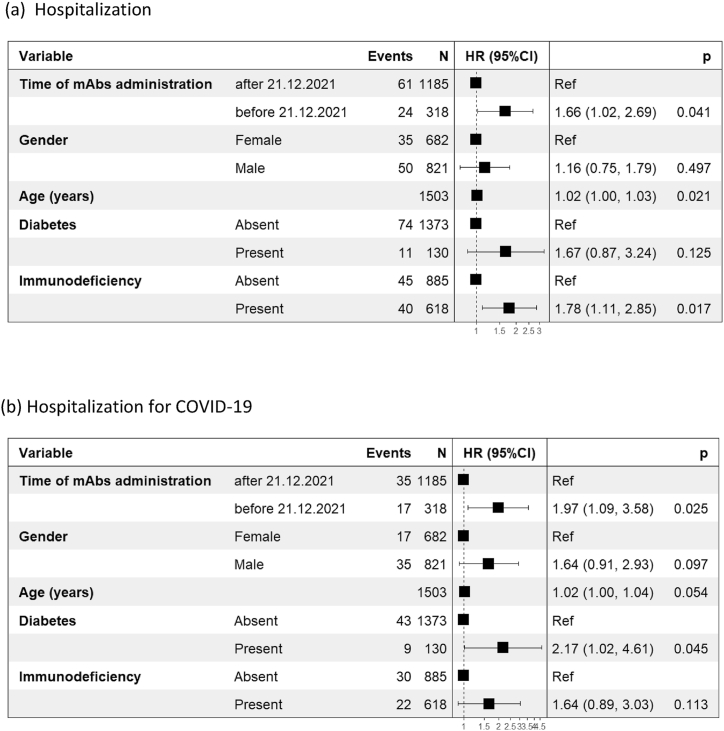
Methods: CONDIVIDIAMO, a two-year multicenter observational study, consecutively enrolled SARS-CoV-2 outpatients with ≥1 risk factor for COVID-19 progression receiving mAbs. Demographic data, underlying medical condition, type of mAbs combination received, duration of symptoms before mAbs administration, COVID-19 vaccination history, were collected upon enrolment and centrally recorded. Data on outcomes (hospitalizations, reasons of hospitalization, deaths) were prospectively collected. The primary endpoint was the rate of hospitalization or death in a 28-day follow-up, whichever occurred first; subjects were censored at the day of last follow-up or up to 28 days. The Kaplan-Meier method was used to estimate the incidence rate curve in time. The Cox regression model was used to assess potential risk factors for unfavorable outcome. Results were shown as hazard ratio (HR) along with the corresponding 95 % Confidence Interval (95%CI).
Results: Among 1534 subjects (median [interquartile range, IQR] age 66.5 [52.4-74.9] years, 693 [45.2 %] women), 632 (41.2 %) received bamlanivimab ± etesevimab, 209 (13.6 %) casirivimab/imdevimab, 586 (38.2 %) sotrovimab, 107 (7.0 %) tixagevimab/cilgavimab. After 28-day follow-up, 87/1534 (5.6 %, 95%CI: 4.4%-6.8 %) met the primary outcome (85 hospitalizations, 2 deaths). Hospitalizations for COVID-19 (52, 3.4 %) occurred earlier than for other reasons (33, 2.1 %), after a median (IQR) of 3.5 (1-7) versus 8 (3-15) days (p = 0.006) from mAbs administration.In a multivariable Cox regression model, factors independently associated with increased hospitalization risk were age (hazard ratio [HR] 1.02, 95%CI 1.00-1.03, p = 0.021), immunodeficiency (HR 1.78, 95%CI 1.11-2.85, p = 0.017), pre-Omicron calendar period (HR 1.66, 95%CI 1.02-2.69, p = 0.041).
Conclusions: MAbs real-world data over a 2-year changing pandemic landscape showed the feasibility of the intervention, although the hospitalization rate was not negligible. Immunosuppressed subjects remain more at risk of clinical worsening.
Keywords: COVID-19; Hospitalization; Immunodeficiency; Monoclonal antibodies; Omicron variant; SARS-CoV-2.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Gandhi R.T., Lynch J.B., Del Rio C. Mild or moderate covid-19. N. Engl. J. Med. 2020;383(18):1757–1766. - PubMed
-
- Berlin D.A., Gulick R.M., Martinez F.J. Severe covid-19. N. Engl. J. Med. 2020;383(25):2451–2460. - PubMed
-
- Gupta A., Gonzalez-Rojas Y., Juarez E., et al. Early treatment for covid-19 with SARS-CoV-2 neutralizing antibody sotrovimab. N. Engl. J. Med. 2021;385(21):1941–1950. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
