

Atrial Fibrillation in Hypertrophic Cardiomyopathy
- PMID: 39247675
- PMCID: PMC11379995
- DOI: 10.1016/j.jacadv.2024.101210
Atrial Fibrillation in Hypertrophic Cardiomyopathy
Abstract
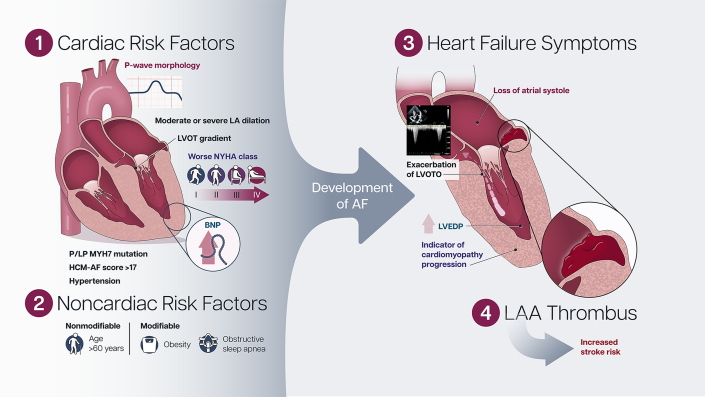
Atrial fibrillation (AF) is common among patients with hypertrophic cardiomyopathy (HCM) with a prevalence greater than 25%. AF in HCM is associated with a high risk of stroke and can be a marker of more advanced cardiomyopathy. Although, it frequently results in cardiac hemodynamic changes which are poorly tolerated, it can be subclinical. Thus, prompt diagnosis and adequate management of AF are essential to minimizing AF-related adverse outcomes in HCM. All HCM patients should be screened for AF regularly, and those with high-risk features should be screened more frequently preferably with extended ambulatory monitoring. Once AF is detected, oral anticoagulation should be initiated. Both general and HCM-specific modifiable risk factors should be addressed and assessment for cardiomyopathy progression should be performed. Although no randomized controlled studies have compared rate versus rhythm control in HCM, early rhythm control could be considered to prevent further LA remodeling.
Keywords: anti-coagulation; atrial fibrillation; hypertrophic cardiomyopathy; rate control; rhythm control.
© 2024 The Authors.
Conflict of interest statement
Dr Weissler-Snir has received speaker fees from Bristol Myer Squibb; and fees for publication steering committee participation for Cytokinetics and research grants from 10.13039/100004374Medtronic. Dr Rader has received consultant and speaker fees from Bristol Myer Squibbs, Medtronic, Recor Medical, and Cytokinetics. Dr Saberi has received consultant/advisor fees from Bristol Myers Squibb; and has received research grants from Bristol Myers Squibb, 10.13039/100014941Cytokinetics, 10.13039/100004336Novartis, and 10.13039/100005646Actelion Pharmaceuticals. Dr Wong is the site principal investigator for clinical trials sponsored by Bristol Myers Squibb, Cytokinetics, and Tenaya Therapeutics; and discloses unpaid advisory board participation for Bristol Myers Squibb and Cytokinetics. Dr Owens has received consulting/research support from 10.13039/100014941Cytokinetics, MyoKardia/Bristol Myers Squibb, Pfizer, Lexicon Pharmaceuticals, Tenaya Therapeutics, Stealth BioTherapeutics, Renovacor, Edgewise Therapeutics, BioMarin Pharmaceuticals, and Lexeo Therapeutics.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
