

Metroticket approach in a retrospective cohort study to predict overall survival after surgical resection for hepatocellular carcinoma
- PMID: 39248314
- PMCID: PMC11573095
- DOI: 10.1097/JS9.0000000000001868
Metroticket approach in a retrospective cohort study to predict overall survival after surgical resection for hepatocellular carcinoma
Abstract
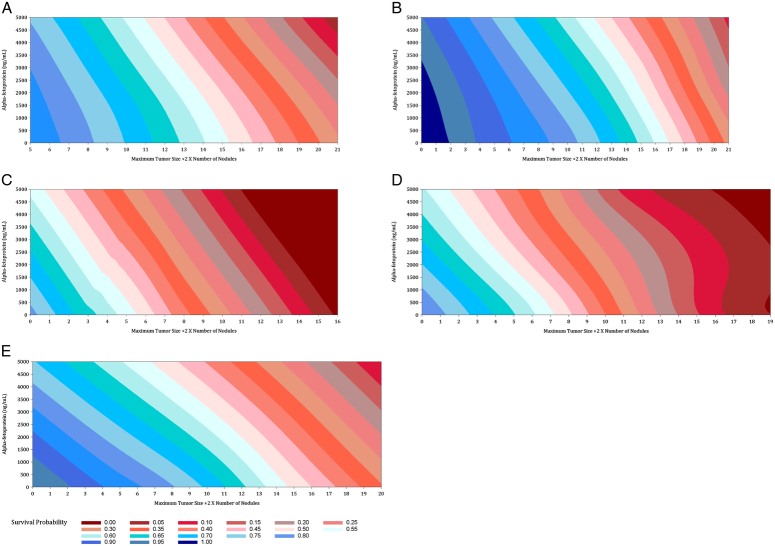
Background: Surgical resection is a curative therapy for early-stage hepatocellular carcinoma (HCC) patients meeting the Milan criteria as well as a widely used therapy in intermediate-stage HCC. However, intermediate-stage HCC encompasses a wide spectrum of disease and there is a lack of good predictive models for the long-term clinical outcome of HCC patients currently. Here, the authors adopt Mazzaferro's Metroticket 2.0 to create a robust survival prediction model for intermediate-stage HCC patients undergoing surgical resection. Our algorithm considers age, AFP levels, ALBI score, and nodule size/number to generate survival estimates in an accessible graph format. Importantly, their model surpasses the American Joint Committee on Cancer staging model and was validated with independent US patient data.
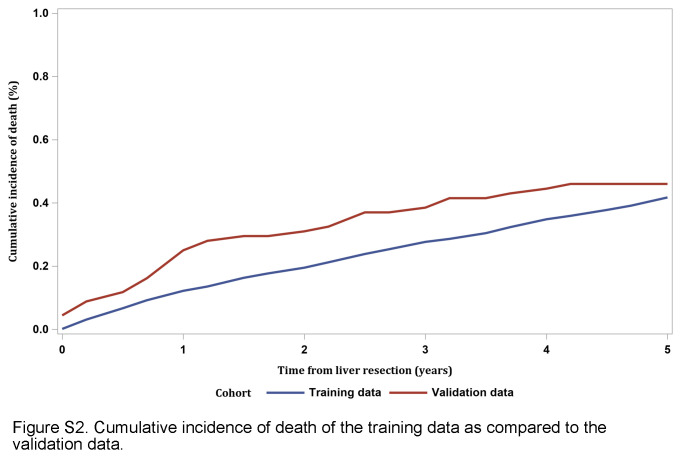
Methods: The authors conducted a retrospective analysis of OS and RFS in early- and intermediate-stage HCC patients treated with liver resection, including a training cohort in Singapore and a validation cohort in North Carolina, USA.
Results: The authors recorded 278 deaths (35.0%) and 428 patients (53.9%) in the first 5 years after surgical resection; higher ALBI score, higher lnAFP, more advanced age and higher tumour burden index were identified as significant parameters. The overall predictive capability of our model, with the inclusion of AFP, is reflected with a UNO's C-statistic of 0.655, which is 1.11 times better than the 0.5895 C-statistic of the 8th AJCC TNM Staging model.
Conclusions: The authors' modified Metroticket model allows for more granular and better-informed prognostication. This will help surgeons and patients make accurate comparisons between the clinical outcomes of surgical resection and other non-surgical treatments.
Trial registration: ClinicalTrials.gov NCT06294808.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures



References
-
- Ferlay JE, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today Lyon. Int Agency Res Cancer 2020.
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet 2012;379:1245–1255. - PubMed
-
- Lim KC, Chow PK, Allen JC, et al. Systematic review of outcomes of liver resection for early hepatocellular carcinoma within the Milan criteria. Br J Surg 2012;99:1622–1629. - PubMed
-
- Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology 2002;35:519–524. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
