

Management of aortic disease in children with FBN1-related Marfan syndrome
- PMID: 39250726
- PMCID: PMC11472455
- DOI: 10.1093/eurheartj/ehae526
Management of aortic disease in children with FBN1-related Marfan syndrome
Abstract
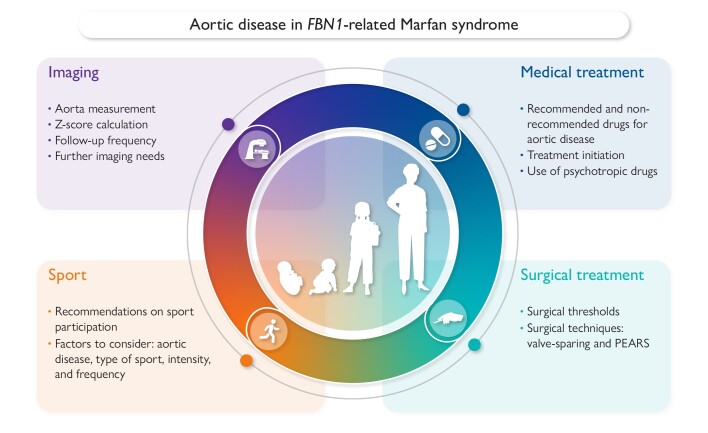
Marfan syndrome (MFS) is a hereditary connective tissue disorder with an estimated prevalence of 1:5000-1:10 000 individuals. It is a pleiotropic disease characterized by specific ocular, cardiovascular, and skeletal features. The most common cardiovascular complication is aortic root dilatation which untreated can lead to life-threatening aortic root dissection, mainly occurring in adult patients. Prompt diagnosis, appropriate follow-up, and timely treatment can prevent aortic events. Currently there are no specific recommendations for treatment of children with MFS, and management is greatly based on adult guidelines. Furthermore, due to the scarcity of studies including children, there is a lack of uniform treatment across different centres. This consensus document aims at bridging these gaps of knowledge. This work is a joint collaboration between the paediatric subgroup of the European Network of Vascular Diseases (VASCERN, Heritable Thoracic Aortic Disease Working Group) and the Association for European Paediatric and Congenital Cardiology (AEPC). A group of experts from 12 different centres and 8 different countries participated in this effort. This document reviews four main subjects, namely, (i) imaging of the aorta at diagnosis and follow-up, (ii) recommendations on medical treatment, (iii) recommendations on surgical treatment, and (iv) recommendations on sport participation.
Keywords: Aortic disease treatment; Aortic imaging; Children; Exercise recommendation; Marfan syndrome.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
