

Effect of sodium-glucose co-transporter-2 inhibitors on survival free of organ support in patients hospitalised for COVID-19 (ACTIV-4a): a pragmatic, multicentre, open-label, randomised, controlled, platform trial
- PMID: 39250922
- PMCID: PMC11451207
- DOI: 10.1016/S2213-8587(24)00218-3
Effect of sodium-glucose co-transporter-2 inhibitors on survival free of organ support in patients hospitalised for COVID-19 (ACTIV-4a): a pragmatic, multicentre, open-label, randomised, controlled, platform trial
Abstract
Background: Patients hospitalised for COVID-19 are at risk for multiorgan failure and death. Sodium-glucose co-transporter-2 (SGLT2) inhibitors provide cardiovascular and kidney protection in patients with cardiometabolic conditions and could provide organ protection during COVID-19. We aimed to investigate whether SGLT2 inhibitors can reduce the need for organ support in patients hospitalised for COVID-19.
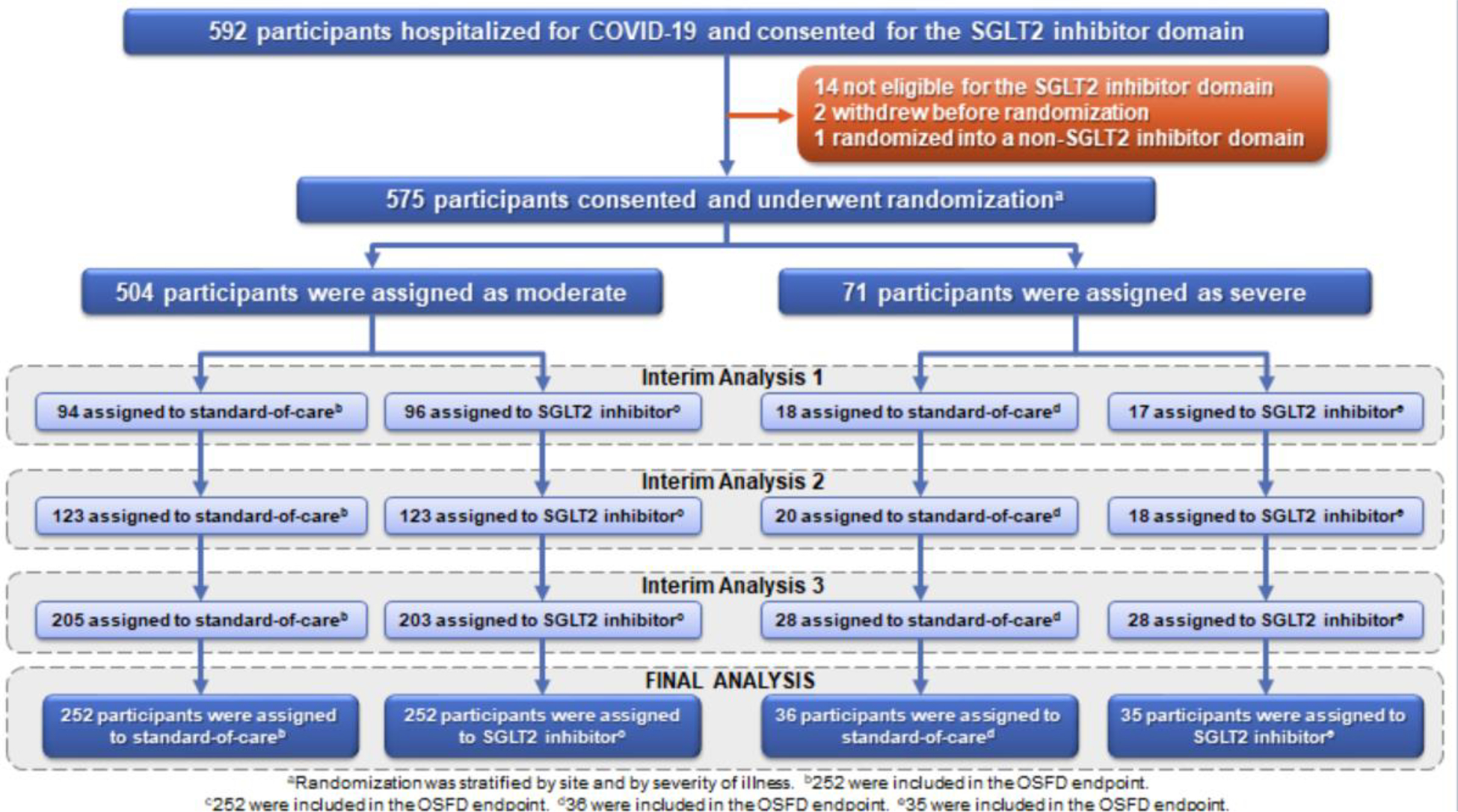
Methods: This pragmatic, multicentre, open-label, randomised, controlled, platform trial was conducted across 63 sites in the USA, Spain, Brazil, Italy, and Mexico. Patients aged at least 18 years hospitalised for COVID-19 (moderate or severe illness) were randomly assigned (1:1), via an interactive voice system or web-response system, to receive locally available SGLT2 inhibitor (administered orally, once daily) plus standard-of-care or standard-of-care for 30 days. The primary outcome was organ support-free days evaluated through 21 days, assessed using intention-to-treat approach. This trial is registered on ClinicalTrials.gov, NCT04505774.
Findings: The first patient was randomly assigned to the SGLT2 inhibitor domain on Dec 3, 2021. On March 31, 2023, at the recommendation of the data and safety monitoring board, enrolment in the SGLT2 inhibitor domain for both moderately and severely ill hospitalised patients was stopped prematurely for futility due to a low likelihood of finding a treatment benefit. The final randomised population consisted of 575 patients (mean age 72 years [SD 13], 242 (42%) female and 154 (27%) Hispanic; 504 in the moderate illness group and 71 in the severe illness group). 573 patients had a known 21-day outcome; 215 (75%) of 285 patients in the SGLT2 inhibitor plus standard-of-care group did not require respiratory or cardiovascular organ support versus 231 (80%) of 288 patients in the standard-of-care group. The adjusted odds ratio (OR) for an SGLT2 inhibitor effect on organ support-free days was 0·74 (95% Credible Interval [CrI] 0·48-1·13; where OR higher than 1 indicated treatment benefit, yielding a posterior probability of futility P(OR <1·2) of 99% and a posterior probability of inferiority P(OR<1·0) of 91%). There were 37 deaths (13%) in the SGLT2 inhibitor plus standard-of-care group and 42 deaths (15%) in the standard-of-care group at 90 days (hazard ratio 0·91 [95% CrI 0·58-1·43], probability of hazard ratio <1 of 66%). No safety concerns were observed with SGLT2 inhibitors, including no cases of ketoacidosis.
Interpretation: SGLT2 inhibitors did not significantly increase days free of organ support or reduce mortality in patients hospitalised with COVID-19. SGLT2 inhibitors were well tolerated with no observed safety concerns. Overall, these findings do not support the use of SGLT2 inhibitors as standard care in patients hospitalised with COVID-19.
Funding: National Institutes of Health.
Copyright © 2024 Elsevier Ltd. All rights reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
Declaration of interests MNK has received research grant support from University of Pittsburgh, AstraZeneca, Boehringer Ingelheim, and Pfizer; has served as a consultant or on an advisory board for 35Pharma, Alnylam, Amgen, Applied Therapeutics, Arrowhead Pharmaceuticals, AstraZeneca, Bayer, Boehringer Ingelheim, Cytokinetics, Dexcom, Eli Lilly, Esperion Therapeutics, Imbria Pharmaceuticals, Janssen, Lexicon Pharmaceuticals, Merck (Diabetes and Cardiovascular), Novo Nordisk, Pharmacosmos, Pfizer, Regeneron, scPharmaceuticals, Structure Therapeutics, Vifor Pharma, and Youngene Therapeutics; has received other research support from AstraZeneca and Vifor Pharma; and has received honoraria from AstraZeneca, Boehringer Ingelheim, and Novo Nordisk. He holds stock options from Artera Health and Saghmos Therapeutics. OV has received institutional research support from AstraZeneca, Bayer, and Cardurion, and has served as a consultant or advisory board member for AstraZeneca, Cardior, Cytokinetics, and Sanofi. JSB reports research grants from National Institutes of Health and American Heart Association and has consulted for Janssen. HRR reports receiving grants from the National Heart, Lung, and Blood Institute during the conduct of the study, as well as nonfinancial support from Abbott Vascular, SHL Telemedicine, Siemens, and Phillips outside the submitted work. ADA is an employee of Medtronic. SDS has received research grants from Alexion, Alnylam, AstraZeneca, Bellerophon, Bayer, BMS, Cytokinetics, Eidos, Gossamer, GSK, Ionis, Lilly, MyoKardia, National Institutes of Health/National Heart, Lung, and Blood Institute, Novartis, NovoNordisk, Respicardia, Sanofi Pasteur, Theracos, US2.AI, and has consulted for Abbott, Action, Akros, Alexion, Alnylam, Amgen, Arena, AstraZeneca, Bayer, Boeringer-Ingelheim, BMS, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi-Sankyo, GSK, Lilly, Merck, Myokardia, Novartis, Roche, Theracos, Quantum Genomics, Cardurion, Janssen, Cardiac Dimensions, Tenaya, Sanofi-Pasteur, Dinaqor, Tremeau, CellProThera, Moderna, American Regent, Sarepta, Lexicon, Anacardio, Akros, and Valo. ASB has received research grant support to his institution from National Institutes of Health/National Heart, Lung, and Blood Institute, National Institutes of Health/National Institute on Aging, American College of Cardiology Foundation, and the Centers for Disease Control and Prevention. AP reports a research grant from the German Research Foundation. MNG reports receiving grants from National Institutes of Health, Agency for Healthcare Research and Quality, and the US Centers for Disease Control and Prevention and receiving personal fees from Regeneron for serving on the data safety monitoring board for monoclonal antibody trials in COVID-19. LZK reports receiving personal fees from Cerus Corp, University of Maryland, Coagulant Therapeutics, Haemonetics, and Gamma Diagnostics. PK receives grant funding as a principal investigator from NIH and Cerenovus; consulting fees as a scientific advisor to Basking Biosciences, Bayer, Lumosa, and Shionogi; and royalties for online publication from UpToDate. KSK reports grants from National Institutes of Health during the conduct of the study, funding from Eisai outside the submitted work, and personal fees from National Institutes of Health for committee service indirectly related to the research. LBK reports that her institution received funding from National Institutes of Health to perform the study. AJ reports receiving funding from AstraZeneca to study mechanisms of action of dapagliflozin. LW reports funding from the National Institutes of Health for ACTIV-4A and ACTIV-4C. JLSM reports receiving honoraria from Roche la Hoffman and Novartis. MQH reports receiving research funding from National Institutes of Health and NIAID. JLS reports research grants or contracts from Amgen, BMS, GSK, Medtronic, Pfizer, Sanofi-Aventis; funding for educational activities or lectures from Pfizer, BMS, Novo Nordisk, AstraZeneca, and funding for consulting from Bayer, Boehringer Ingelheim, BMS, Novo Nordisk, and AstraZeneca. RDL has received grants from Amgen, BMS, and GSK; consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, BMS, and NovoNordisk; and Honoraria from AstraZeneca, Daiichi Sankyo, NovoNordisk and Pfizer. JLC reports direct support for this project from National Institutes of Health/National Heart, Lung, and Blood Institute; grants from National Institutes of Health/National Heart, Lung, and Blood Institute, National Institutes of Health/NIAID, the Department of Defense, the Department of Veterans Affairs, and the COPD Foundation, outside of this project; and support paid to his institution outside this project from CDL Behring, LLC, AstraZeneca, and Novartis, GBMH. B-AK (through SOCAR Research) received grants from National Institutes of Health. MWG reports funding in part by the National Institutes of Health Agreement 1OT2HL156812 through the National Heart, Lung, and Blood Institute CONNECTS programme. MDN serves as chief medical officer for Haima Therapeutics and has received grants from the National Heart, Lung, and Blood Institute, National Institute of General Medical Sciences, Department of Defense, Haemonetics, and Instrumentation Laboratories. He has received personal fees from Haemonetics, Takeda, CSL Behring, and Janssen Pharmaceuticals. JSH is the study chair for ACTIV-4a under a National Heart, Lung, and Blood Institute–University of Pittsburgh grant subaward. SLW, SB, JFL, ESL, ALK, MC, CC, and AA declare no competing interests.
Figures


Comment in
-
Sodium-glucose co-transporter type-2 inhibitors for hospitalised patients with COVID-19: safe but not protective.Lancet Diabetes Endocrinol. 2024 Oct;12(10):685-687. doi: 10.1016/S2213-8587(24)00230-4. Epub 2024 Sep 6. Lancet Diabetes Endocrinol. 2024. PMID: 39250920 No abstract available.
References
-
- Usman MS, Siddiqi TJ, Anker SD, et al. Effect of SGLT2 Inhibitors on Cardiovascular Outcomes Across Various Patient Populations. J Am Coll Cardiol 2023; 81(25): 2377–2387. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
