

Characterization of postintensive care syndrome in a prospective cohort of survivors of COVID-19 critical illness: a 12-month follow-up study
- PMID: 39251486
- PMCID: PMC11408405
- DOI: 10.1007/s12630-024-02811-4
Characterization of postintensive care syndrome in a prospective cohort of survivors of COVID-19 critical illness: a 12-month follow-up study
Abstract
Purpose: Studies integrating an exhaustive longitudinal long-term follow-up of postintensive care syndrome (PICS) in critically ill COVID-19 survivors are scarce. We aimed to 1) describe PICS-related sequelae over a 12-month period after intensive care unit (ICU) discharge, 2) identify relevant demographic and clinical factors related to PICS, and 3) explore how PICS-related sequelae may influence health-related quality of life (HRQoL) in critically ill COVID-19 survivors.
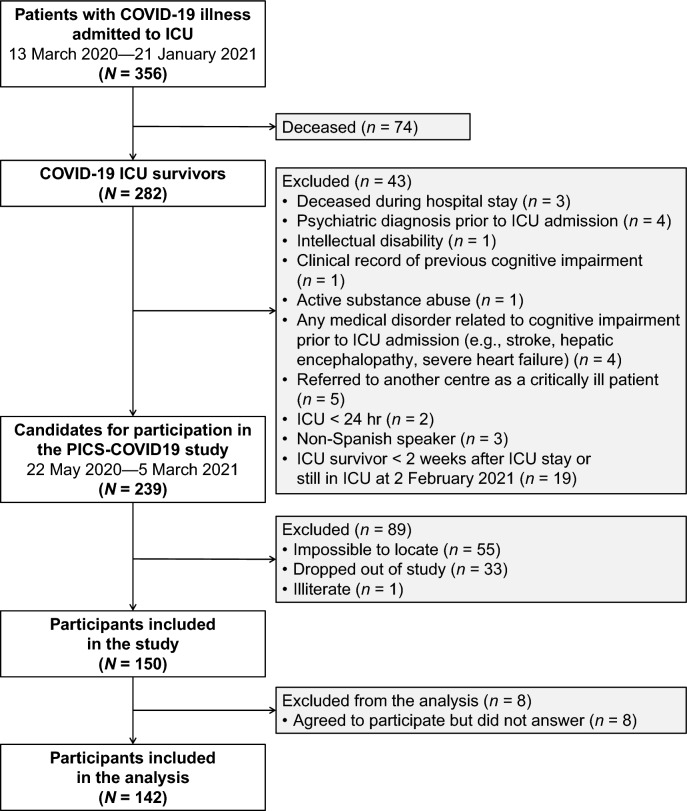
Methods: We conducted a prospective cohort study in adult critically ill survivors of SARS-CoV-2 infection that did or did not need invasive mechanical ventilation (IMV) during the COVID-19 pandemic in Spain (March 2020 to January 2021). We performed a telemedicine follow-up of PICS-related sequelae (physical/functional, cognitive, and mental health) and HRQoL with five data collection points. We retrospectively collected demographic and clinical data. We used multivariable mixed-effects models for data analysis.
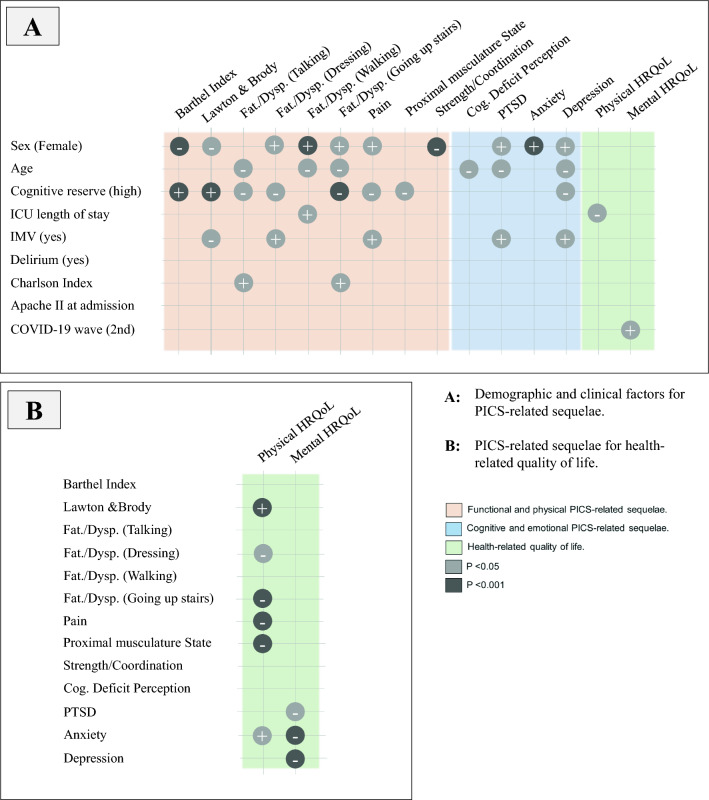
Results: We included 142 study participants in the final analysis, with a median [interquartile range] age of 61 [53-68] yr; 35% were female and 59% needed IMV. Fatigue/dyspnea, pain, impaired muscle function, psychiatric symptomatology and reduced physical HRQoL were prominent sequelae early after ICU discharge. Over the 12-month follow-up, functionality and fatigue/dyspnea improved progressively, while pain remained stable. We observed slight fluctuations in anxiety symptoms and perception of cognitive deficit, whereas posttraumatic stress disorder (PTSD) and depressive symptoms improved, with a mild rebound at the end of the follow-up. Female sex, younger age, and the need for IMV were risk factors for PICS, while having higher cognitive reserve was a potential protective factor. Physical HRQoL scores showed a general improvement over time, whereas mental HRQoL remained stable. Shorter ICU stay, better functionality, and lower scores for fatigue/dyspnea and pain were associated with better physical HRQoL, while lower scores for anxiety, depression, and PTSD were associated with better mental HRQoL.
Conclusions: Postintensive care syndrome was common in COVID-19 critical illness survivors and persisted in a significant proportion of patients one year after ICU discharge, impacting HRQoL. The presence of risk factors for PICS may identify patients who are more likely to develop the condition and who would benefit from more specific and closer follow-up after ICU admission.
Study registration: ClinicalTrials.gov ( NCT04422444 ); first submitted 9 June 2020.
RéSUMé: OBJECTIF: Les études intégrant un suivi longitudinal exhaustif à long terme des syndromes post-soins intensifs (SPSI) chez les survivant·es gravement malades de la COVID-19 sont rares. Notre objectif était 1) de décrire les séquelles liées au SPSI sur une période de 12 mois après la sortie de l’unité de soins intensifs (USI), 2) d’identifier les facteurs démographiques et cliniques pertinents liés au SPSI, et 3) d’explorer comment les séquelles liées au SPSI peuvent influencer la qualité de vie liée à la santé (QVLS) chez les survivant·es gravement malades de la COVID-19. MéTHODE: Nous avons mené une étude de cohorte prospective chez des adultes gravement malades survivant·es d’une infection par le SRAS-CoV-2 qui ont eu ou non besoin d’une ventilation mécanique invasive (VMI) pendant la pandémie de COVID-19 en Espagne (mars 2020 à janvier 2021). Nous avons effectué un suivi par télémédecine des séquelles liées au SPSI (santé physique/fonctionnelle, cognitive et mentale) et à la QVLS avec cinq points de collecte de données. Nous avons rétrospectivement colligé des données démographiques et cliniques. Des modèles multivariés à effets mixtes ont été utilisés pour l’analyse des données. RéSULTATS: Nous avons inclus 142 participant·es à l’étude dans l’analyse finale, avec un âge médian [intervalle interquartile] de 61 [53-68] ans; 35 % étaient des femmes et 59 % avaient besoin de VMI. La fatigue/dyspnée, la douleur, l’altération de la fonction musculaire, la symptomatologie psychiatrique et la réduction de la QVLS physique étaient des séquelles importantes peu après la sortie de l’USI. Au cours du suivi de 12 mois, la fonctionnalité et la fatigue/dyspnée se sont améliorées progressivement, tandis que la douleur est restée stable. Nous avons observé de légères fluctuations des symptômes d’anxiété et de perception du déficit cognitif, tandis que le trouble de stress post-traumatique (ESPT) et les symptômes dépressifs se sont améliorés, avec un léger rebond à la fin du suivi. Le sexe féminin, un jeune âge et le besoin de VMI étaient des facteurs de risque de SPSI, tandis qu’une réserve cognitive plus élevée était un facteur potentiel de protection. Les scores physiques de la QVLS ont montré une amélioration générale au fil du temps, tandis que la QVLS mentale est restée stable. Un séjour plus court aux soins intensifs, une meilleure fonctionnalité et des scores plus faibles pour la fatigue/dyspnée et la douleur étaient associés à une meilleure QVLS physique, tandis que des scores plus faibles pour l’anxiété, la dépression et le ESPT étaient associés à une meilleure QVLS mentale. CONCLUSION: Le syndrome post-soins intensifs était fréquent chez les survivant·es d’une maladie grave de la COVID-19 et a persisté chez une proportion importante de patient·es un an après leur sortie de l’unité de soins intensifs, ce qui a eu un impact sur la QVLS. La présence de facteurs de risque de SPSI peut identifier les patient·es qui sont plus susceptibles de développer la maladie et qui bénéficieraient d’un suivi plus spécifique et plus étroit après leur admission aux soins intensifs. ENREGISTREMENT DE L’éTUDE: ClinicalTrials.gov ( NCT04422444 ); première soumission le 9 juin 2020.
Keywords: COVID-19; critical care; intensive care unit; neuropsychiatric sequelae; physical outcomes; postintensive care syndrome; quality of life; telemedicine assessment.
© 2024. The Author(s).
Conflict of interest statement
All authors declare no conflict of interests.
Figures

References
-
- Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit. Crit Care Med 2012; 40: 502–9. 10.1097/ccm.0b013e318232da75 - PubMed
-
- Herridge MS, Moss M, Hough CL, et al. Recovery and outcomes after the acute respiratory distress syndrome (ARDS) in patients and their family caregivers. Intensive Care Med 2016; 42: 725–38. 10.1007/s00134-016-4321-8 - PubMed
MeSH terms
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
