

Uric acid and alterations of purine recycling disorders in Parkinson's disease: a cross-sectional study
- PMID: 39251680
- PMCID: PMC11385569
- DOI: 10.1038/s41531-024-00785-0
Uric acid and alterations of purine recycling disorders in Parkinson's disease: a cross-sectional study
Abstract
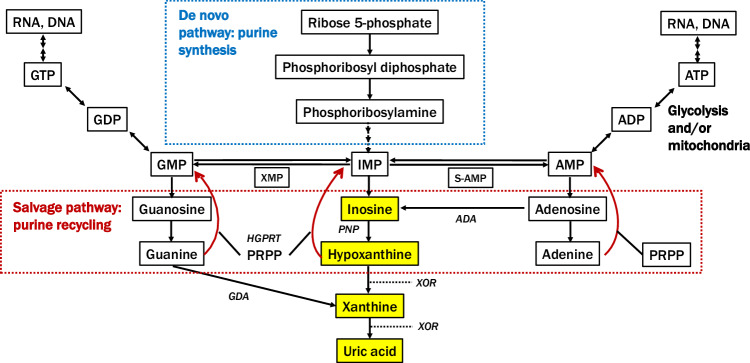
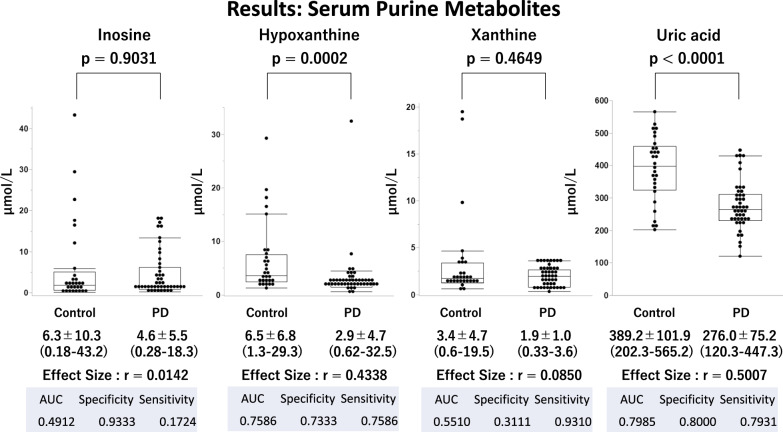
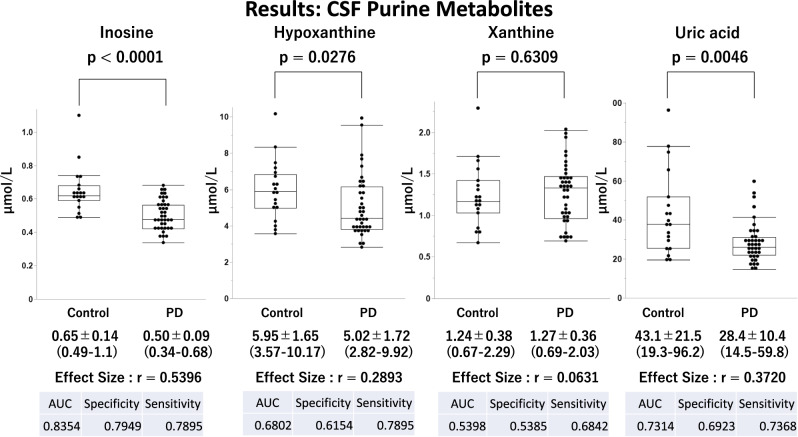
The relationship between reduced serum uric acid (UA) levels and Parkinson's disease (PD), particularly purine metabolic pathways, is not fully understood. Our study compared serum and cerebrospinal fluid (CSF) levels of inosine, hypoxanthine, xanthine, and UA in PD patients and healthy controls. We analyzed 132 samples (serum, 45 PD, and 29 age- and sex-matched healthy controls; CSF, 39 PD, and 19 age- and sex-matched healthy controls) using liquid chromatography-tandem mass spectrometry. Results showed significantly lower serum and CSF UA levels in PD patients than in controls (p < 0.0001; effect size r = 0.5007 in serum, p = 0.0046; r = 0.3720 in CSF). Decreased serum hypoxanthine levels were observed (p = 0.0002; r = 0.4338) in PD patients compared to controls with decreased CSF inosine and hypoxanthine levels (p < 0.0001, r = 0.5396: p = 0.0276, r = 0.2893). A general linear model analysis indicated that the reduced UA levels were mainly due to external factors such as sex and weight in serum and age and weight in CSF unrelated to the purine metabolic pathway. Our findings highlight that decreased UA levels in PD are influenced by factors beyond purine metabolism, including external factors such as sex, weight, and age, emphasizing the need for further research into the underlying mechanisms and potential therapeutic approaches.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
