

A pan-cancer dye for solid-tumour screening, resection and wound monitoring via short-wave and near-infrared fluorescence imaging
- PMID: 39251765
- PMCID: PMC11699565
- DOI: 10.1038/s41551-024-01248-w
A pan-cancer dye for solid-tumour screening, resection and wound monitoring via short-wave and near-infrared fluorescence imaging
Abstract
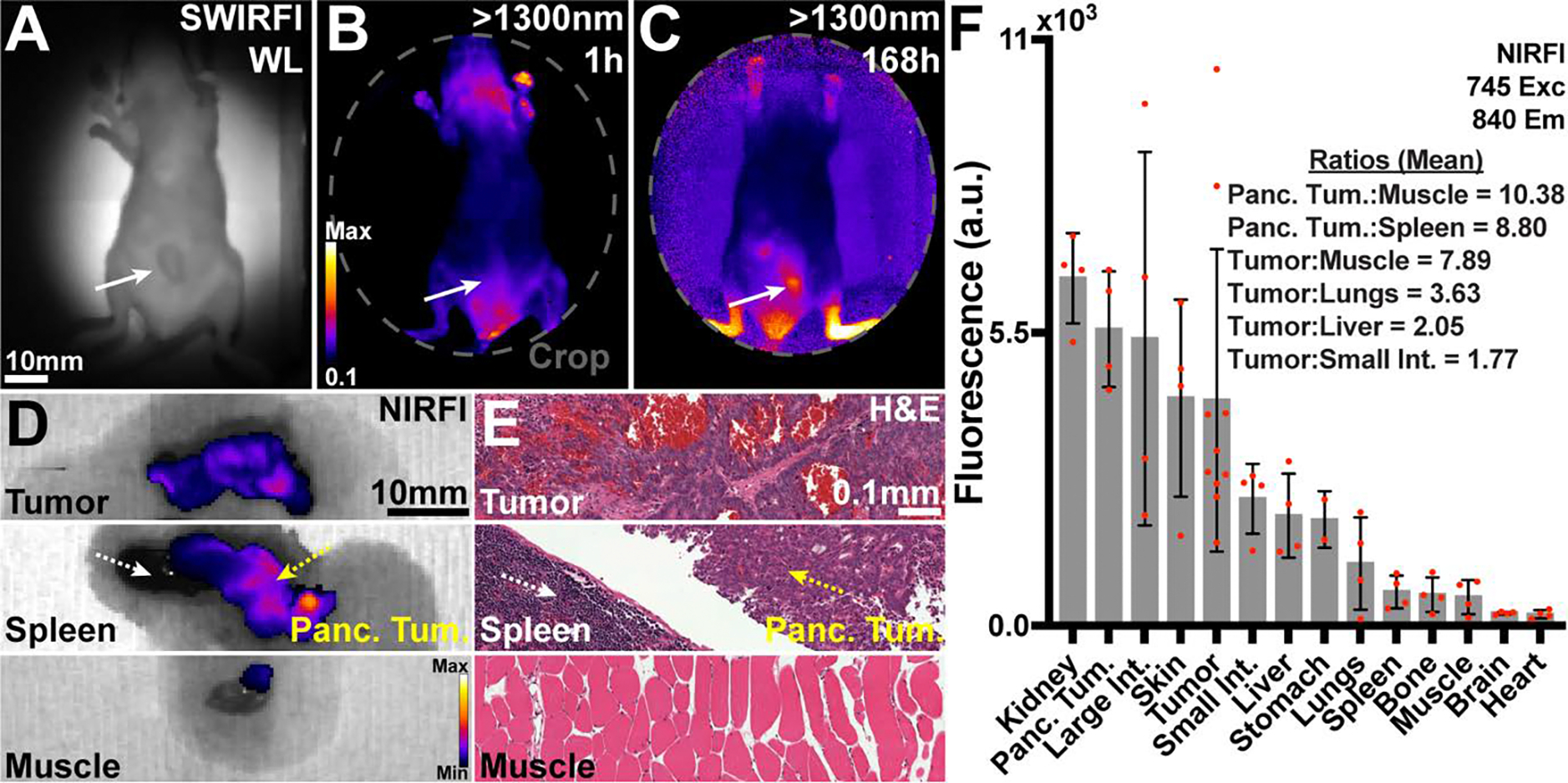
The efficacy of fluorescence-guided surgery in facilitating the real-time delineation of tumours depends on the optical contrast of tumour tissue over healthy tissue. Here we show that CJ215-a commercially available, renally cleared carbocyanine dye sensitive to apoptosis, and with an absorption and emission spectra suitable for near-infrared fluorescence imaging (wavelengths of 650-900 nm) and shortwave infrared (SWIR) fluorescence imaging (900-1,700 nm)-can facilitate fluorescence-guided tumour screening, tumour resection and the assessment of wound healing. In tumour models of either murine or human-derived breast, prostate and colon cancers and of fibrosarcoma, and in a model of intraperitoneal carcinomatosis, imaging of CJ215 with ambient light allowed for the delineation of nearly all tumours within 24 h after intravenous injection of the dye, which was minimally taken up by healthy organs. At later timepoints, CJ215 provided tumour-to-muscle contrast ratios up to 100 and tumour-to-liver contrast ratios up to 18. SWIR fluorescence imaging with the dye also allowed for quantifiable non-contact wound monitoring through commercial bandages. CJ215 may be compatible with existing and emerging clinical solutions.
© 2024. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Figures







Update of
-
A pan-cancer agent for screening, resection and wound monitoring via NIR and SWIR imaging.Res Sq [Preprint]. 2024 Jan 23:rs.3.rs-3879635. doi: 10.21203/rs.3.rs-3879635/v1. Res Sq. 2024. Update in: Nat Biomed Eng. 2024 Sep;8(9):1092-1108. doi: 10.1038/s41551-024-01248-w. PMID: 38343820 Free PMC article. Updated. Preprint.
References
-
- Li M et al. 800CW Dye and 89Zr Dual-labeled Antibody for the PET/NIRF/Cerenkov Multi-modality Imaging of ICAM-1 (CD54) in Pancreatic Cancer. Journal of Nuclear Medicine 60, 331–331 (2019).
MeSH terms
Substances
Grants and funding
- R56 EB030512/EB/NIBIB NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- T32 GM141949/GM/NIGMS NIH HHS/United States
- R00-EB033580/U.S. Department of Health & Human Services | NIH | National Institute of Biomedical Imaging and Bioengineering (NIBIB)
- R01 CA215719/CA/NCI NIH HHS/United States
- R01 CA257811/CA/NCI NIH HHS/United States
- R01 EB033651/EB/NIBIB NIH HHS/United States
- R01-EB033651/U.S. Department of Health & Human Services | NIH | National Institute of Biomedical Imaging and Bioengineering (NIBIB)
- R00 EB033580/EB/NIBIB NIH HHS/United States
- R01-CA215719/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
LinkOut - more resources
Full Text Sources
