

Efficacy and safety of angiotensin receptor-neprilysin inhibition in heart failure patients with end-stage kidney disease on maintenance dialysis: A systematic review and meta-analysis
- PMID: 39252524
- PMCID: PMC11798635
- DOI: 10.1002/ejhf.3454
Efficacy and safety of angiotensin receptor-neprilysin inhibition in heart failure patients with end-stage kidney disease on maintenance dialysis: A systematic review and meta-analysis
Abstract
Aims: Angiotensin receptor-neprilysin inhibitor (ARNI) has played an increasingly important role in the management of heart failure (HF). However, the evidence on the benefits of ARNI in HF patients with end-stage kidney disease (ESKD) undergoing dialysis is limited. This study aimed to investigate the efficacy and safety of ARNI in patients with concomitant HF and ESKD on maintenance dialysis.
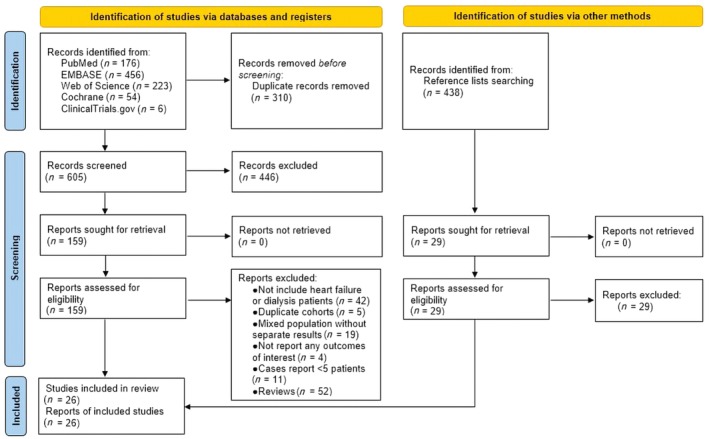
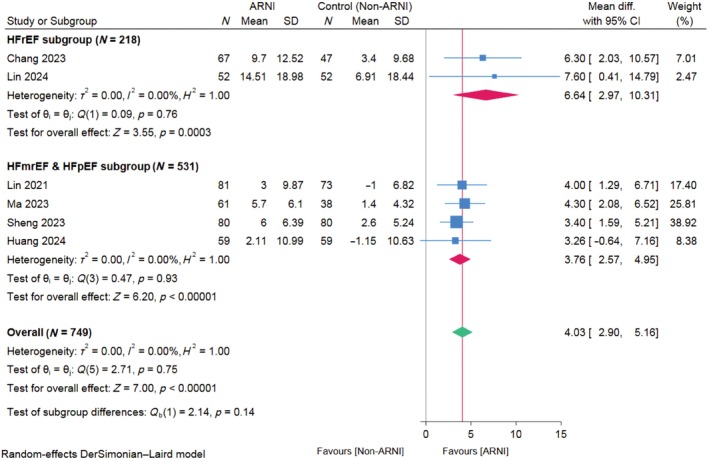
Methods and results: We systematically searched the MEDLINE, Embase, Web of Science, Cochrane, and ClinicalTrials.gov databases for studies reporting outcomes after ARNI treatment in HF patients with ESKD on dialysis. All meta-analyses were performed using the random effects model. Twenty-six studies comprising 2494 patients with concomitant HF and ESKD undergoing dialysis were included. Our synthesis showed a significant improvement in left ventricular ejection fraction (LVEF) between before and after ARNI treatment (mean change: 8.05%; 95% confidence interval [CI] 5.57-10.54). Compared to the conventional group, the ARNI group showed a greater improvement in LVEF (mean difference: 4.03%; 95% CI 2.90-5.16). This effect was more pronounced in patients with HF with reduced ejection fraction (pinteraction < 0.0001). Patients treated with ARNI had a lower risk of all-cause mortality (risk ratio [RR] 0.64; 95% CI 0.45-0.92; p = 0.01) but had a similar rate of HF hospitalization (RR 0.71; 95% CI 0.43-1.18; p = 0.19). ARNI treatment showed benefits in the improvement of left ventricular end-systolic diameter, left ventricular mass index, left atrial diameter, and E/e' ratio (p < 0.05), while it did not significantly increase the risk of severe hyperkalaemia (p = 0.33) or symptomatic hypotension (p = 0.53).
Conclusion: This meta-analysis provided insights into the benefits of ARNI in HF patients with ESKD undergoing dialysis by improving left ventricular function, reversing left ventricular remodelling, and reducing the risk of all-cause mortality, without increasing the risk of HF hospitalizations, severe hyperkalaemia, and symptomatic hypotension.
Keywords: Angiotensin receptor–neprilysin inhibitor; Dialysis; End‐stage kidney disease; Heart failure; Meta‐analysis; Sacubitril/valsartan.
© 2024 The Author(s). European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
