

Integrating cardiovascular risk assessment into mobile low-dose CT lung screenings in rural Appalachia: A comprehensive analysis of the relationship between lung cancer risk, coronary artery calcium burden, and cardiovascular risk reduction strategies
- PMID: 39252854
- PMCID: PMC11381835
- DOI: 10.1016/j.ajpc.2024.100719
Integrating cardiovascular risk assessment into mobile low-dose CT lung screenings in rural Appalachia: A comprehensive analysis of the relationship between lung cancer risk, coronary artery calcium burden, and cardiovascular risk reduction strategies
Abstract
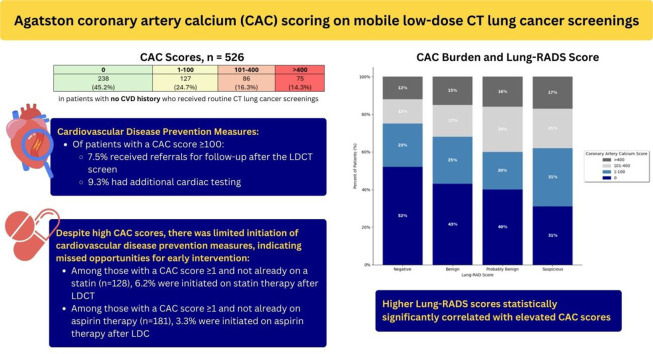
Objective: Mobile low-dose computed tomography (LDCT) lung screenings are part of an outreach program in rural Appalachia to detect early lung cancer. Coronary artery calcium (CAC) scoring on LDCT can identify calcium deposits in coronary arteries and can prompt consideration of risk modification for prevention of cardiovascular disease (CVD) events. It is not known if Lung CT Screening Reporting & Data System (Lung-RADS) scoring correlates with CAC scores. There is no clear guidance for patients undergoing LDCT screenings to receive follow-up regarding CAC or prevention of associated CVD risk.
Methods: This was a retrospective review of mobile LDCT LCS in adults with no known history of CVD. CT images were obtained at 100 kVp with a slice thickness of 3 mm. Agatston CAC scoring was performed retroactively. Lung-RADS scores were categorized as: Negative (1), Benign (2), Probably Benign (3), and Suspicious (4). CAC scoring was grouped as 0, 1-100, 101-399, and ≥400. Descriptive statistics and chi-square analyses were utilized.
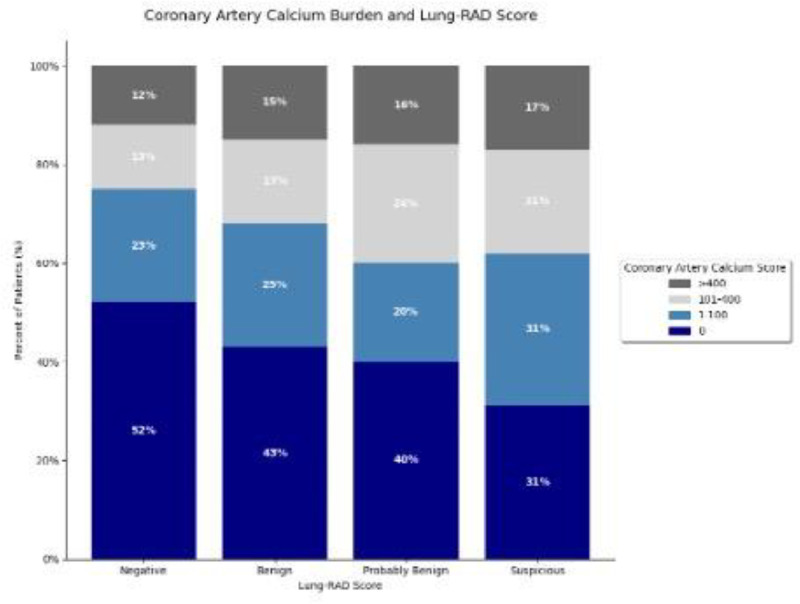
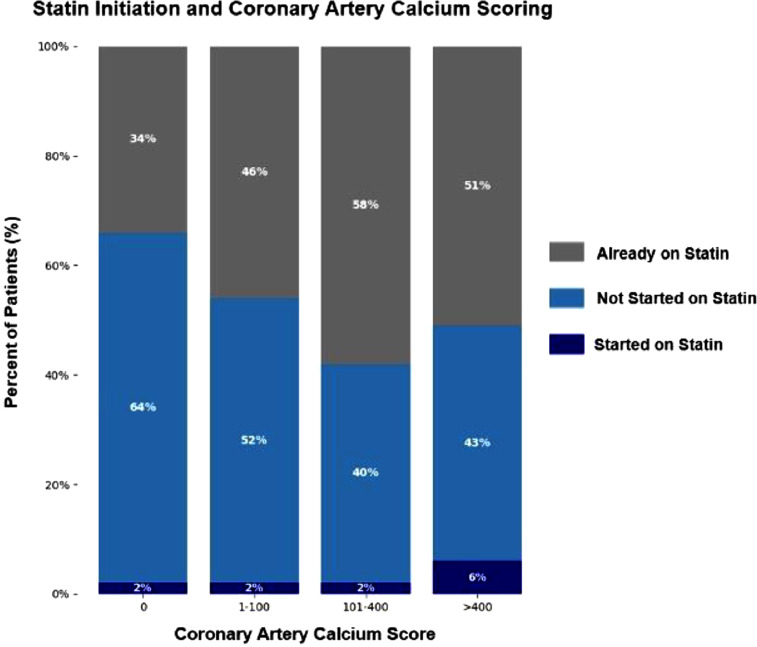
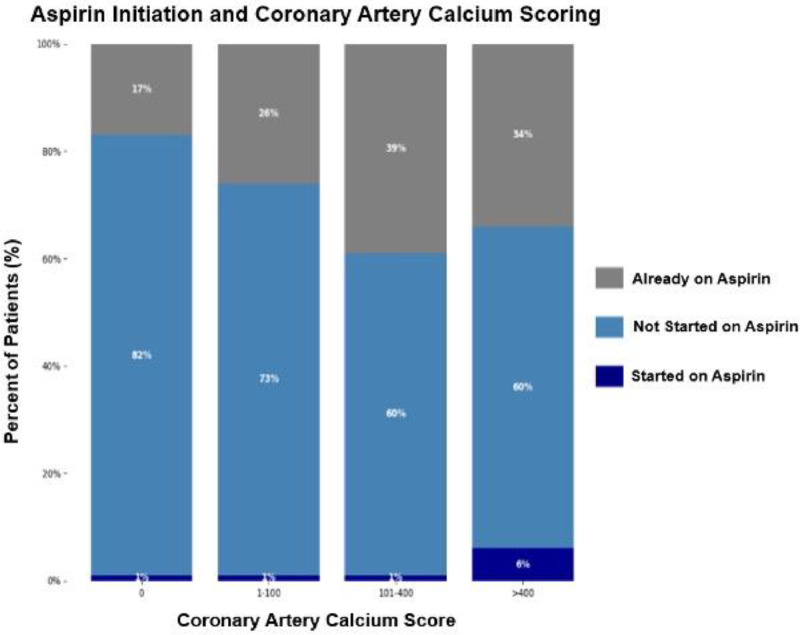
Results: A total of 526 LDCT screenings were included. Over 54 % of patients had coronary calcification on LDCT LCS. 161 patients (30.6 %) had a CAC score of ≥100 and 75 patients (14.3 %) had a CAC score ≥400. Of patients with a CAC score ≥100, 7.5 % received referrals for follow-up after the LDCT screen and 9.3 % had additional cardiac testing. Of those with a CAC score ≥100 not already on a statin (45.3 %) and not already on aspirin (63.3 %), few were started within 3 months of LDCT for prevention (8.2 % and 5.9 % respectively). Among patients with a Lung-RADS score of 4, 17 % had a CAC score >400, whereas only 12 % with a Lung-RADS score of 1 fell into the same CAC category. Higher Lung-RADS scores correlated with fewer patients with CAC of 0. A significant correlation was observed between higher Lung-RADS scores and elevated CAC scores (p = 0.02).
Conclusion: In patients with no CVD history, coronary artery calcification was frequently identified on mobile LDCT lung screenings in rural communities. Patients with higher probabilities of malignant lung nodules may also be at increased risk for significant coronary artery disease. Calcium scoring from LDCT screenings allowed for simultaneous assessment of lung cancer and CVD risk. Unfortunately, few referrals or CVD prevention medications were initiated. Awareness of CAC score utility, follow-up for identified coronary calcifications, and consideration of primary prevention medications when indicated, would be beneficial in patients undergoing LDCT lung screenings, especially in rural areas with limited healthcare access.
Keywords: Cardiovascular disease prevention; Coronary artery calcium score; Lung-RADS.
© 2024 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
The Future of Concurrent Automated Coronary Artery Calcium Scoring on Screening Low-Dose Computed Tomography.Cureus. 2020 Jun 12;12(6):e8574. doi: 10.7759/cureus.8574. Cureus. 2020. PMID: 32670710 Free PMC article. Review.
-
Reliability analysis of visual ranking of coronary artery calcification on low-dose CT of the thorax for lung cancer screening: comparison with ECG-gated calcium scoring CT.Int J Cardiovasc Imaging. 2014 Dec;30 Suppl 2:81-7. doi: 10.1007/s10554-014-0507-8. Epub 2014 Aug 2. Int J Cardiovasc Imaging. 2014. PMID: 25084979
-
Reporting Coronary Artery Calcium on Low-Dose Computed Tomography Impacts Statin Management in a Lung Cancer Screening Population.Fed Pract. 2022 Sep;39(9):382-388. doi: 10.12788/fp.0318. Epub 2022 Sep 14. Fed Pract. 2022. PMID: 36583089 Free PMC article.
-
Coronary calcium score and emphysema extent on different CT radiation dose protocols in lung cancer screening.Eur Radiol. 2025 Jul;35(7):3781-3787. doi: 10.1007/s00330-024-11254-w. Epub 2024 Dec 20. Eur Radiol. 2025. PMID: 39704802 Free PMC article.
-
Extracoronary Thoracic and Coronary Artery Calcifications on Chest CT for Lung Cancer Screening: Association with Established Cardiovascular Risk Factors - The "CT-Risk" Trial.Acad Radiol. 2015 Jul;22(7):880-9. doi: 10.1016/j.acra.2015.03.005. Epub 2015 May 7. Acad Radiol. 2015. PMID: 25957500 Review.
Cited by
-
The Role of Computed Tomography and Artificial Intelligence in Evaluating the Comorbidities of Chronic Obstructive Pulmonary Disease: A One-Stop CT Scanning for Lung Cancer Screening.Int J Chron Obstruct Pulmon Dis. 2025 May 6;20:1395-1406. doi: 10.2147/COPD.S508775. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40352362 Free PMC article. Review.
-
AI-Enhanced CAD in Low-Dose CT: Balancing Accuracy, Efficiency, and Overdiagnosis in Lung Cancer Screening.Thorac Cancer. 2025 Jan;16(1):e15499. doi: 10.1111/1759-7714.15499. Epub 2024 Nov 27. Thorac Cancer. 2025. PMID: 39600243 Free PMC article. No abstract available.
References
-
- Hecht Harvey S., et al. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: a report of the society of cardiovascular computed tomography and society of thoracic radiology. J Cardiovasc Comput Tomogr. 2017;11(1):74–84. - PubMed
-
- Anon. West Virginia. 2023, https://www.cdc.gov/nchs/pressroom/states/westvirginia/wv.htm.
-
- Anon, LUCAS Wvucancer. 2023 https://cancer.wvumedicine.org/about-us/programs/mobile-cancer-screening... Accessed.
-
- Allen Amy R., et al. Addressing lung cancer health disparities in west Virginia: an academic-industry collaboration model. J Health Care Poor Underserved. 2022;33(4S):173–179. - PubMed
LinkOut - more resources
Full Text Sources
