

This is a preprint.
Natural History, Phenotype Spectrum and Clinical Outcomes of Desmin (DES)-Associated Cardiomyopathy
- PMID: 39252922
- PMCID: PMC11383507
- DOI: 10.1101/2024.08.24.24311904
Natural History, Phenotype Spectrum and Clinical Outcomes of Desmin (DES)-Associated Cardiomyopathy
Update in
-
Natural History, Phenotype Spectrum, and Clinical Outcomes of Desmin (DES)-Associated Cardiomyopathy.Circ Genom Precis Med. 2025 Apr;18(2):e004878. doi: 10.1161/CIRCGEN.124.004878. Epub 2025 Feb 19. Circ Genom Precis Med. 2025. PMID: 39968648
Abstract
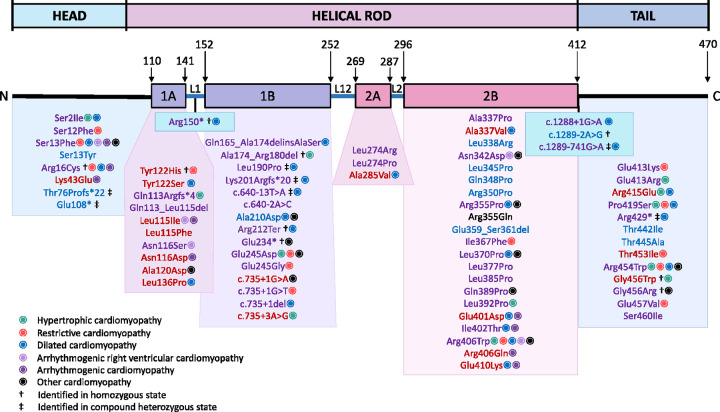
Background: Pathogenic/likely pathogenic (P/LP) desmin (DES) variants cause heterogeneous cardiomyopathy and/or skeletal myopathy phenotypes. Limited data suggest a high incidence of major adverse cardiac events (MACE), including cardiac conduction disease (CCD), sustained ventricular arrhythmias (VA), and heart failure (HF) events (HF hospitalization, LVAD/cardiac transplant, HF-related death), in patients with P/LP DES variants. However, pleiotropic presentation and small cohort sizes have limited clinical phenotype and outcome characterization.
Objectives: We aimed to describe the natural history, phenotype spectrum, familial penetrance and outcomes in patients with P/LP DES variants through a systematic review and individual patient data meta-analysis using published reports.
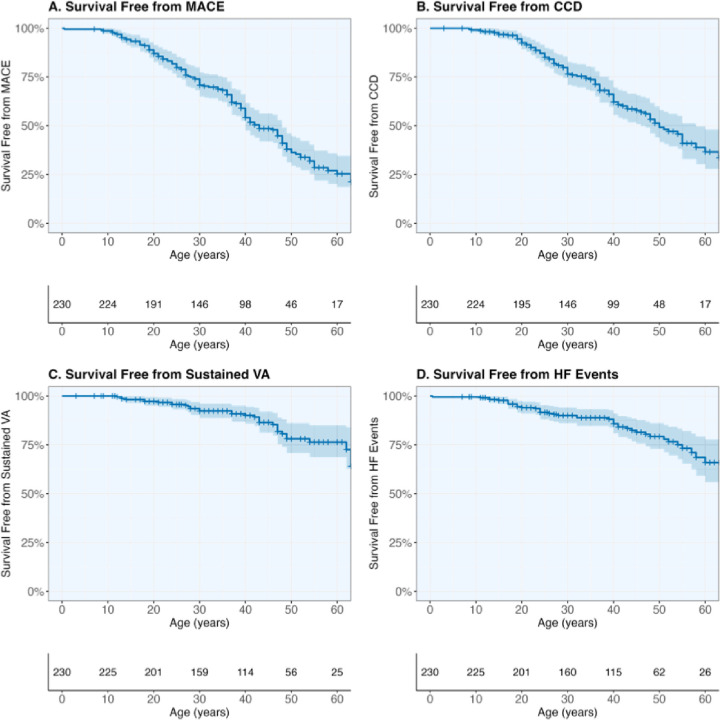
Methods: We searched Medline (PubMed) and Embase for studies that evaluated cardiac phenotypes in patients with P/LP DES variants. Cardiomyopathy diagnosis or occurrence of MACE were considered evidence of cardiac involvement/penetrance. Lifetime event-free survival from CCD, sustained VA, HF events, and composite MACE was assessed.
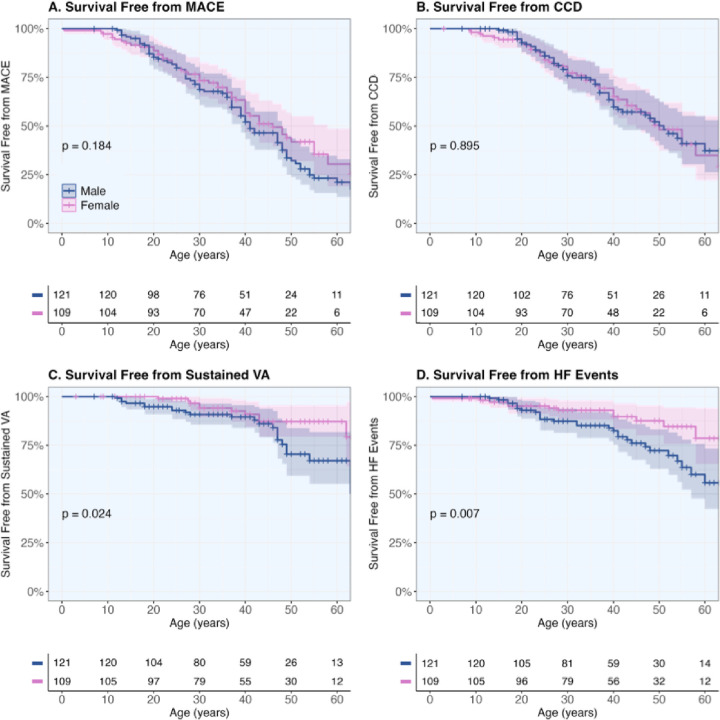
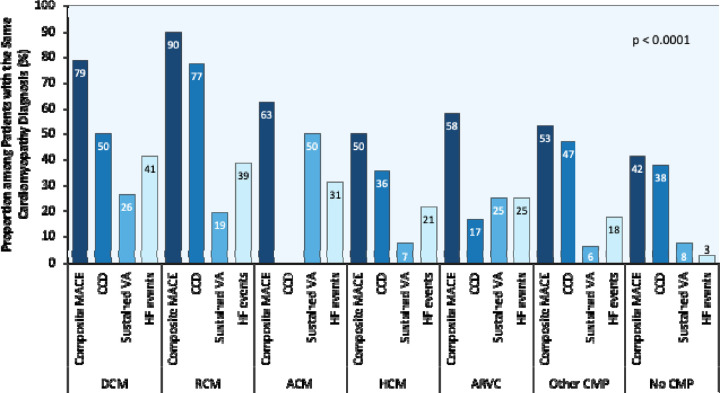
Results: Out of 4,212 screened publications, 71 met the inclusion criteria. A total of 230 patients were included (52.6% male, 52.2% probands, median age: 31 years [22.0; 42.8] at first evaluation, median follow-up: 3 years [0; 11.0]). Overall, 124 (53.9%) patients were diagnosed with cardiomyopathy, predominantly dilated cardiomyopathy (14.8%), followed by restrictive cardiomyopathy (13.5%), whereas other forms were less common: arrhythmogenic cardiomyopathy (7.0%), hypertrophic cardiomyopathy (6.1%), arrhythmogenic right ventricular cardiomyopathy (5.2%), and other forms (7.4%). Overall, 132 (57.4%) patients developed MACE, with 96 [41.7%] having CCD, 36 [15.7%] sustained VA, and 43 [18.7%] HF events. Familial penetrance of cardiac disease was 63.6% among relatives with P/LP DES variants. Male sex was associated with increased risk of sustained VA (HR 2.28, p=0.02) and HF events (HR 2.45, p=0.008).
Conclusions: DES cardiomyopathy exhibits heterogeneous phenotypes and distinct natural history, characterized by high familial penetrance and substantial MACE burden. Male patients face higher risk of sustained VA events.
Keywords: cardiac arrhythmia; cardiomyopathy; genetics; genomics; penetrance; precision medicine; prognosis; risk stratification; sudden cardiac death.
Figures
References
-
- Pieperhoff S, Borrmann C, Grund C, Barth M, Rizzo S, Franke WW. The area composita of adhering junctions connecting heart muscle cells of vertebrates. VII. The different types of lateral junctions between the special cardiomyocytes of the conduction system of ovine and bovine hearts. Eur J Cell Biol 2010;89:365–78. - PubMed
-
- van Spaendonck-Zwarts KY, van Hessem L, Jongbloed JD et al. Desmin-related myopathy. Clin Genet 2011;80:354–66. - PubMed
-
- Segura-Rodriguez D, Bermudez-Jimenez FJ, Carriel V et al. Myocardial fibrosis in arrhythmogenic cardiomyopathy: a genotype-phenotype correlation study. Eur Heart J Cardiovasc Imaging 2020;21:378–386. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous