

Renin-Angiotensin System Inhibition in Patients With Myocardial Injury Complicating Transcatheter Aortic Valve Replacement
- PMID: 39253713
- PMCID: PMC11381816
- DOI: 10.1016/j.jacadv.2024.101212
Renin-Angiotensin System Inhibition in Patients With Myocardial Injury Complicating Transcatheter Aortic Valve Replacement
Abstract
Background: Periprocedural myocardial injury impacts clinical outcome after transcatheter aortic valve replacement (TAVR). The optimal medical management strategy for TAVR-related periprocedural myocardial injury has not been established.
Objectives: The authors aimed to investigate the prognostic association of renin-angiotensin system (RAS) inhibitors in patients with periprocedural myocardial injury after TAVR.
Methods: In a prospective TAVR registry, patients were retrospectively stratified according to Valve Academic Research Consortium (VARC)-3 periprocedural myocardial injury and RAS inhibitor prescription after TAVR. The main outcomes of interest were prevalence of myocardial injury and cardiovascular death. Logistic and Cox proportional hazards regression were used to analyze outcomes of interest.
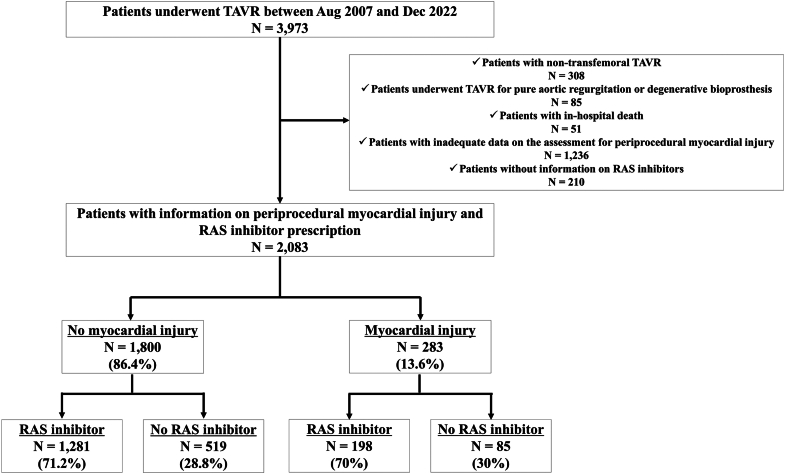
Results: Among 2,083 eligible patients undergoing TAVR between August 2007 and June 2023, 283 patients (13.8%) developed VARC-3 periprocedural myocardial injury. RAS inhibitors were prescribed in 197 patients (70%) with periprocedural myocardial injury and in 1,251 patients (71.2%) without injury. Compared with patients without periprocedural myocardial injury, patients with myocardial injury had an increased risk of cardiovascular death at 1 year (HRadjusted: 2.08; 95% CI: 1.39-3.11). The use of RAS inhibitors after TAVR was associated with a reduced risk of cardiovascular death in patients with and without periprocedural myocardial injury (HRadjusted: 0.46; 95% CI: 0.22-0.95, and HRadjusted: 0.44; 95% CI: 0.30-0.65, respectively).
Conclusions: One out of 7 patients undergoing TAVR experienced periprocedural myocardial injury. VARC-3 periprocedural myocardial injury was associated with a 2-fold increased risk of cardiovascular death at 1 year after TAVR. The favorable association of RAS inhibitor prescription was consistent in patients with and without periprocedural myocardial injury. (SwissTAVI Registry; NCT01368250).
Keywords: Valve Academic Research Consortium; aortic stenosis; periprocedural myocardial injury; renin-angiotensin system inhibitors; transcatheter aortic valve replacement.
© 2024 The Authors.
Conflict of interest statement
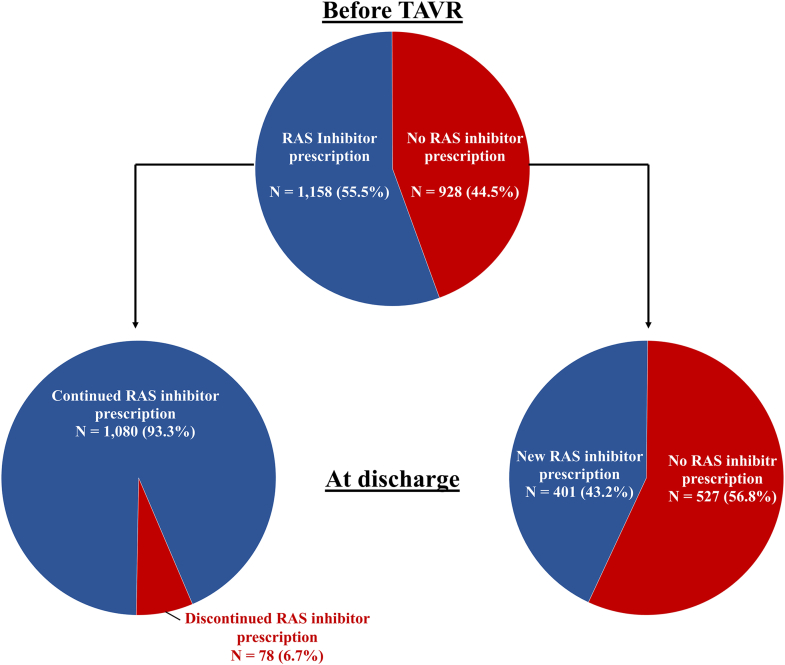
Dr Pilgrim has received research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the Swiss Polar Institute, and the Bangerter-Rhyner Foundation. Research; travel or educational grants to the institution without personal remuneration from Biotronik, Boston Scientific, Edwards Lifesciences, and ATSens; and speaker fees and consultancy fees to the institution from Biotronik, Boston Scientific, Edwards Lifesciences, Abbott, Medtronic, Biosensors, and Highlife. Dr Windecker has received research, travel, or educational grants to the institution without personal remuneration from Abbott, Abiomed, Amgen, AstraZeneca, Bayer, Braun, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardinal Health, CardioValve, Cordis Medical, Corflow Therapeutics, CSL Behring, Daiichi Sankyo, Edwards Lifesciences, Farapulse Inc Fumedica, Guerbet, Idorsia, Inari Medical, InfraRedx, Janssen-Cilag, Johnson & Johnson, Medalliance, Medicure, Medtronic, Merck Sharp & Dohm, Miracor Medical, MonarQ, Novartis, Novo Nordisk, Organon, OrPha Suisse, and Pharming Tech. Pfizer, Polares, Regeneron, Sanofi-Aventis, Servier, Sinomed, Terumo, Vifor, V-Wave. He served as advisory board member and/or member of the steering/executive group of trials funded by 10.13039/100000046Abbott, 10.13039/100020297Abiomed, 10.13039/100002429Amgen, 10.13039/100004325AstraZeneca, 10.13039/100004326Bayer, 10.13039/100008497Boston Scientific, 10.13039/501100005035Biotronik, Bristol Myers Squibb, 10.13039/100006520Edwards Lifesciences, 10.13039/501100023518MedAlliance, 10.13039/100004374Medtronic, 10.13039/100004336Novartis, Polares, Recardio, Sinomed, 10.13039/501100008645Terumo, and V-Wave with payments to the institution but no personal payments and is also member of the steering/executive committee group of several investigator-initiated trials that receive funding by industry without impact on his personal remuneration. Dr Reineke reports travel expenses from Abbott, Edwards Lifesciences, and Medtronic. Dr Stortecky reports research grants to the institution from 10.13039/100006520Edwards Lifesciences, 10.13039/100004374Medtronic, 10.13039/100008497Boston Scientific, and 10.13039/100000046Abbott and personal fees from Boston Scientific, Teleflex, and BTG. Dr Lanz reports speaker fees to the institution from Edwards Lifesciences and Abbott and served as advisory board member for Abbott. Dr Samim received funding for an online course from 10.13039/100006520Edwards Lifesciences. Dr Heg reports and with Department of Clinical Research, University of Bern, which has a staff policy of not accepting honoraria or consultancy fees. However, DCR is involved in design, conduct, or analysis of clinical studies funded by not-for-profit and for-profit organizations. In particular, pharmaceutical and medical device companies provide direct funding to some of these studies. For an up-to-date list of our conflicts of interest see https://www.ctu.unibe.ch/research_projects/declaration_of_interest/index_eng.html. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.PerspectivesCOMPETENCY IN MEDICAL KNOWLEDGE: A recent study suggested that periprocedural myocardial injury according to the VARC-3 criteria more accurately delineates the incidence and prognostic association of periprocedural myocardial injury. However, the optimal medical treatment strategy after periprocedural myocardial injury has not been established. In a prospective TAVR registry, VARC-3 periprocedural myocardial injury was documented in 1 out of 7 patients undergoing TAVR and was associated with a 2-fold increased risk of cardiovascular mortality at 1 year. Prescription of RAS inhibitors was associated with a reduced risk of 1-year mortality after TAVR. A non-negligible proportion of patients were not prescribed RAS inhibitors after TAVR even after development of periprocedural myocardial injury. TRANSLATIONAL OUTLOOK: Further studies are warranted to determine the optimal treatment strategy of patients with severe aortic stenosis undergoing TAVR complicated by myocardial injury.
Figures



References
-
- Otto C.M., Nishimura R.A., Bonow R.O., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2021;77:e25–e197. - PubMed
-
- Vahanian A., Beyersdorf F., Praz F., et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561–632. - PubMed
-
- Kappetein A.P., Head S.J., Généreux P., et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;60:1438–1454. - PubMed
-
- Stundl A., Schulte R., Lucht H., et al. Periprocedural myocardial injury depends on transcatheter heart valve type but does not predict mortality in patients after transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2017;10:1550–1560. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
