

Lipidomic biomarkers in plasma correlate with disease severity in adrenoleukodystrophy
- PMID: 39256476
- PMCID: PMC11387402
- DOI: 10.1038/s43856-024-00605-9
Lipidomic biomarkers in plasma correlate with disease severity in adrenoleukodystrophy
Abstract
Background: X-linked adrenoleukodystrophy (ALD) is a neurometabolic disorder caused by pathogenic variants in ABCD1 resulting very long-chain fatty acids (VLCFA) accumulation in plasma and tissues. Males can present with various clinical manifestations, including adrenal insufficiency, spinal cord disease, and leukodystrophy. Female patients typically develop spinal cord disease and peripheral neuropathy. Predicting the clinical outcome of an individual patient remains impossible due to the lack of genotype-phenotype correlation and predictive biomarkers.
Methods: The availability of a large prospective cohort of well-characterized patients and associated biobank samples allowed us to investigate the relationship between lipidome and disease severity in ALD. We performed a lipidomic analysis of plasma samples from 24 healthy controls, 92 male and 65 female ALD patients.
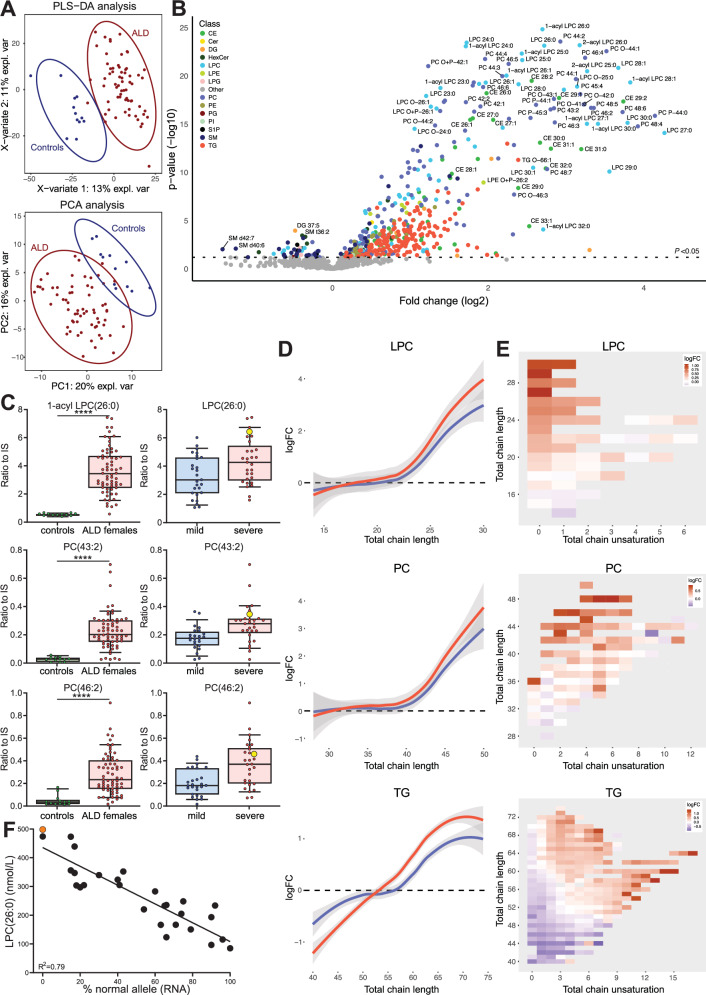
Results: Here we show that VLCFA are incorporated into different lipid classes, including lysophosphatidylcholines, phosphatidylcholines, triglycerides, and sphingomyelins. Our results show a strong association between higher levels of VLCFA-containing lipids and the presence of leukodystrophy, adrenal insufficiency, and severe spinal cord disease in male ALD patients. In female ALD patients, VLCFA-lipid levels correlate with X-inactivation patterns in blood mononuclear cells, and higher levels are associated with more severe disease manifestations. Finally, hematopoietic stem cell transplantation significantly reduces, but does not normalize, plasma C26:0-lysophosphatidylcholine levels in male ALD patients. Our findings are supported by the concordance of C26:0-lysophosphatidylcholine and total VLCFA analysis with the lipidomics results.
Conclusions: This study reveals the profound impact of ALD on the lipidome and provides potential biomarkers for predicting clinical outcomes in ALD patients.
Plain language summary
X-linked adrenoleukodystrophy (ALD) affects the brain, spinal cord, and adrenal glands. ALD is caused by too many very long-chain fatty acids (VLCFAs) in the body. We don’t know how ALD progresses in individual patients. We have analyzed blood samples from male and female ALD patients. We found that certain changes in fatty acid (or lipid) composition are associated with more severe symptoms. Our findings may lead to new ways to predict which symptoms are likely to change over time and to monitor the effectiveness of treatment. This research increases our understanding of ALD and may improve patient care in the future.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Grants and funding
LinkOut - more resources
Full Text Sources
