

Exploration of different statistical approaches in the comparison of dopamine and norepinephrine in the treatment of shock: SOAP II
- PMID: 39256813
- PMCID: PMC11385121
- DOI: 10.1186/s13054-024-05016-9
Exploration of different statistical approaches in the comparison of dopamine and norepinephrine in the treatment of shock: SOAP II
Abstract
Background: Exploring clinical trial data using alternative methods may enhance original study's findings and provide new insights. The SOAP II trial has been published more than 10 years ago; but there is still some speculation that some patients may benefit from dopamine administration for shock management. We aimed to reanalyse the trial under different approaches and evaluate for heterogeneity in treatment effect (HTE).
Methods: All patients enrolled in SOAP II were eligible for reanalysis. We used a variety of methods including the win-ratio (WR), a Bayesian reanalysis stratified according to shock type, and both a risk-based and effect-based explorations for HTE. The methods were applied to different endpoints, including a hierarchy of death, new use of renal-replacement therapy (RRT), and new-onset arrhythmia; 28-day mortality; a composite endpoint (mortality, new use of RRT, and new-onset arrhythmia), and days alive and free of ICU at 28-days (DAFICU28).
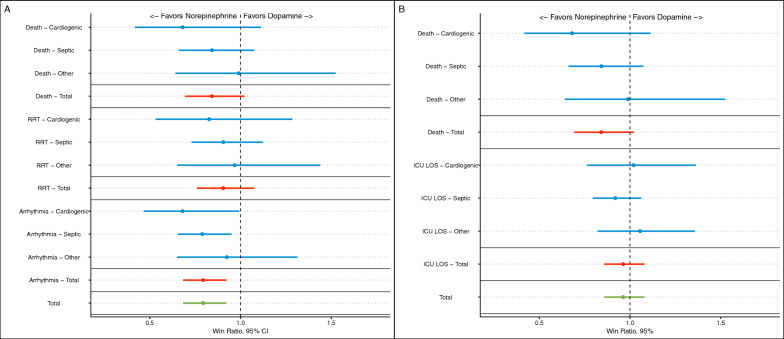
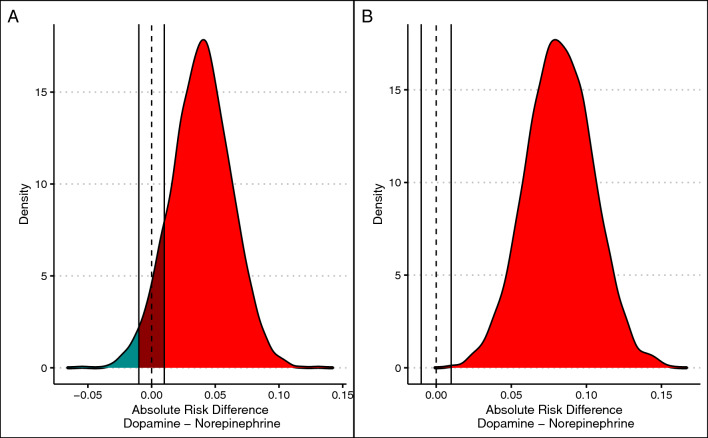
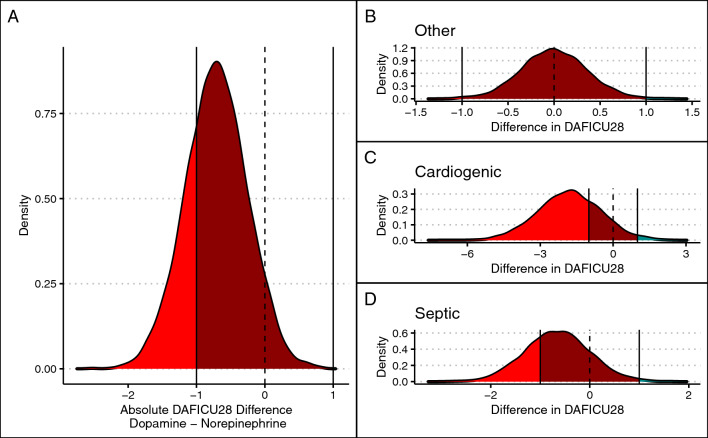
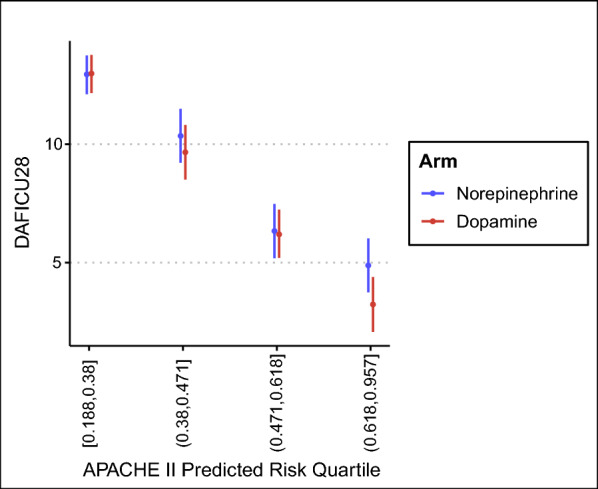
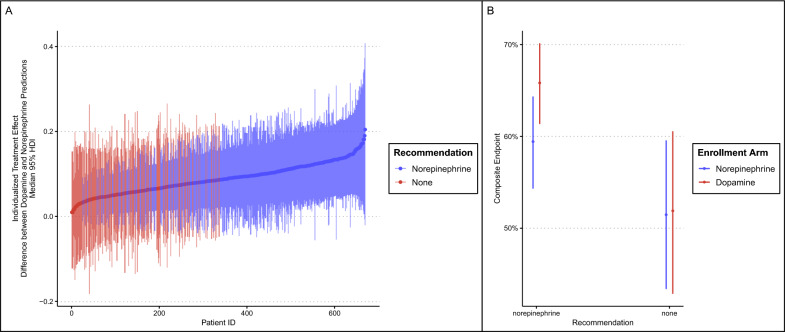
Results: A total of 1679 patients were included (average age was 64.9 years, 57% male, 62% with septic and 17% with cardiogenic shock). All analysis favoured norepinephrine over dopamine. Under the WR approach, dopamine had fewer wins compared to norepinephrine (WR 0.79; 95% confidence intervals [CI] 0.68-0.92; p = 0.003), evident in both cardiogenic and septic shock subgroups. The Bayesian reanalysis for type of shock showed, for dopamine, a probability of harm of 0.95 for mortality, > 0.99 probability of harm for composite endpoint, and 0.91 probability of harm for DAFICU28. The fewer DAFICU28 with dopamine was more apparent in those with cardiogenic shock (0.92). Under the risk-based HTE, there was a high probability that dopamine resulted fewer DAFICU28 in the highest quartile of predicted mortality risk. The effect-based HTE assessment model did not recommended dopamine over norepinephrine for any combination of possible modifiers including age, type of shock, presence of cardiomyopathy, and SOFA score. Receiving dopamine when the effect-based model recommended norepinephrine was associated with an absolute increase in composite endpoint of 6%.
Conclusion: The harm associated with the use of dopamine for the management of shock appears to be present in both septic and cardiogenic shock patients. There was no suggestion of any subgroup in which dopamine was found to be favourable over norepinephrine.
Keywords: Bayesian; Critical care; Dopamine; Norepinephrine; Randomized; Shock.
© 2024. The Author(s).
Conflict of interest statement
Prof Jean-Louis Vincent is Critical Care´s journal editor. FGZ has received personal consulting fees from Baxter and Bactiguard (Sweden), unrelated to the scope of this article.
Figures
References
-
- Rui Q, Jiang Y, Chen M, Zhang N, Yang H, Zhou Y. Dopamine versus norepinephrine in the treatment of cardiogenic shock: a PRISMA-compliant meta-analysis. Medicine. 2017;96(43):e8402. 10.1097/MD.0000000000008402.PMID:29069037;PMCID:PMC5671870. 10.1097/MD.0000000000008402.PMID:29069037;PMCID:PMC5671870 - DOI - PMC - PubMed
-
- De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent JL, SOAP II Investigators. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010;362(9):779–89. 10.1056/NEJMoa0907118. 10.1056/NEJMoa0907118 - DOI - PubMed
-
- Zampieri FG, Casey JD, Shankar-Hari M, Harrell FE Jr, Harhay MO. Using bayesian methods to augment the interpretation of critical care trials. An overview of theory and example reanalysis of the alveolar recruitment for acute respiratory distress syndrome trial. Am J Respir Crit Care Med. 2021;203(5):543–52. 10.1164/rccm.202006-2381CP. 10.1164/rccm.202006-2381CP - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
