

Endogenous tPA levels: A biomarker for discriminating hemorrhagic stroke from ischemic stroke and stroke mimics
- PMID: 39257037
- PMCID: PMC11572725
- DOI: 10.1002/acn3.52197
Endogenous tPA levels: A biomarker for discriminating hemorrhagic stroke from ischemic stroke and stroke mimics
Abstract
Objective: Stroke is the leading cause of death and disability. Timely differentiation between ischemic stroke, hemorrhagic stroke, and stroke mimics is critical for tailored treatment and triage. To accelerate the identification of stroke's subtype, we propose to use the levels of circulating tPA as a biomarker.
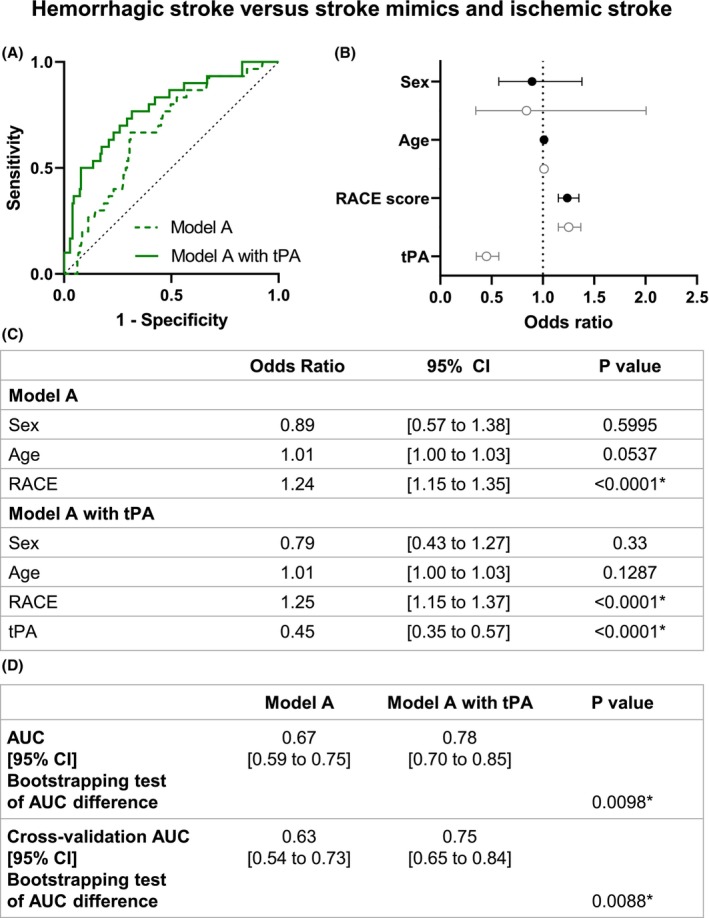
Methods: Biostroke is an observational study performed at the Caen Hospital. We quantified tPA levels in 110 patients with ischemic strokes, 30 patients with hemorrhagic strokes, and 67 stroke mimic patients upon their arrival at the emergency. Two logistic regression models were formulated: one with parameters measurable in an ambulance (Model A) and one with parameters measurable at the hospital (Model H). These models were both tested with or without plasma tPA measurements. Our initial assessment involved evaluating the effectiveness of both models in distinguishing between hemorrhagic strokes, ischemic strokes, and stroke mimics within our study cohort.
Results: Plasmatic tPA levels exhibit significant distinctions between hemorrhagic, ischemic, and mimic stroke patients (1.8; 2.5; 2.4 ng/mL, respectively). The inclusion of tPA in model A significantly enhances the classification accuracy of hemorrhagic patients only, increasing identification from 0.67 (95% CI, 0.59 to 0.75) to 0.78 (95% CI, 0.7 to 0.85) (p = 0.0098). Similarly, in model H, classification accuracy of hemorrhagic patients significantly increased with the addition of tPA, rising from 0.75 (95% CI, 0.67 to 0.83) without tPA to 0.86 (95% CI, 0.81 to 0.91) with tPA (p = 0.024).
Interpretations: Our findings underscore the valuable role of tPA levels in distinguishing between stroke subtypes.
© 2024 The Author(s). Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors declare no conflicts of interests.
Figures







References
-
- Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization (WSO): global stroke fact sheet 2022. Int J Stroke. 2022;17(1):18‐29. - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics‐2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153‐e639. - PubMed
-
- McClelland G, Rodgers H, Flynn D, Price CI. The frequency, characteristics and aetiology of stroke mimic presentations: a narrative review. Eur J Emerg Med. 2019;26(1):2‐8. - PubMed
-
- Liberman AL, Prabhakaran S. Stroke chameleons and stroke mimics in the emergency department. Curr Neurol Neurosci Rep. 2017;17(2):15. - PubMed
-
- Menon BK, Singh N, Sylaja PN. Tenecteplase use in patients with acute ischaemic stroke. Lancet. 2023;401(10377):618‐619. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical