

This is a preprint.
Amiloride Sensitizes Prostate Cancer Cells to the Reversible Tyrosine Kinase Inhibitor Lapatinib by Modulating ERBB3 Subcellular Localization
- PMID: 39257973
- PMCID: PMC11384790
- DOI: 10.21203/rs.3.rs-4844371/v1
Amiloride Sensitizes Prostate Cancer Cells to the Reversible Tyrosine Kinase Inhibitor Lapatinib by Modulating ERBB3 Subcellular Localization
Update in
-
Amiloride sensitizes prostate cancer cells to the reversible tyrosine kinase inhibitor lapatinib by modulating Erbb3 subcellular localization.Cell Mol Life Sci. 2024 Dec 27;82(1):24. doi: 10.1007/s00018-024-05540-5. Cell Mol Life Sci. 2024. PMID: 39725713 Free PMC article.
Abstract
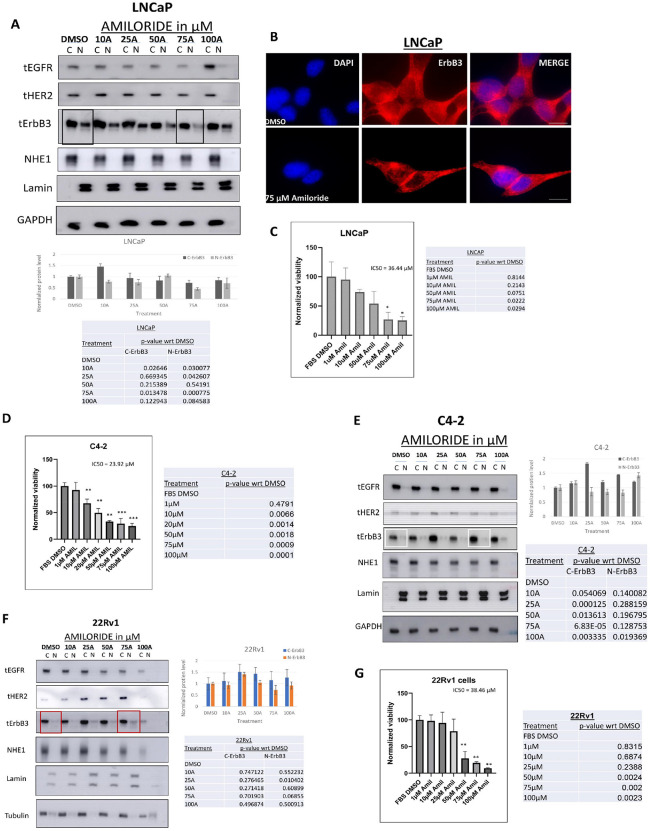
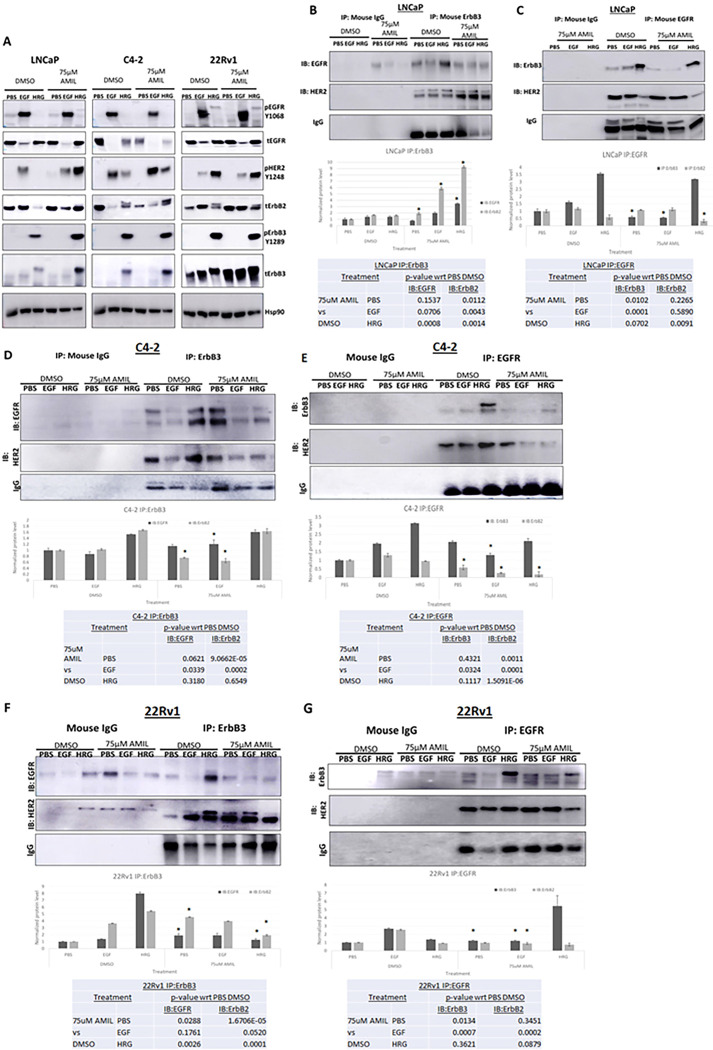
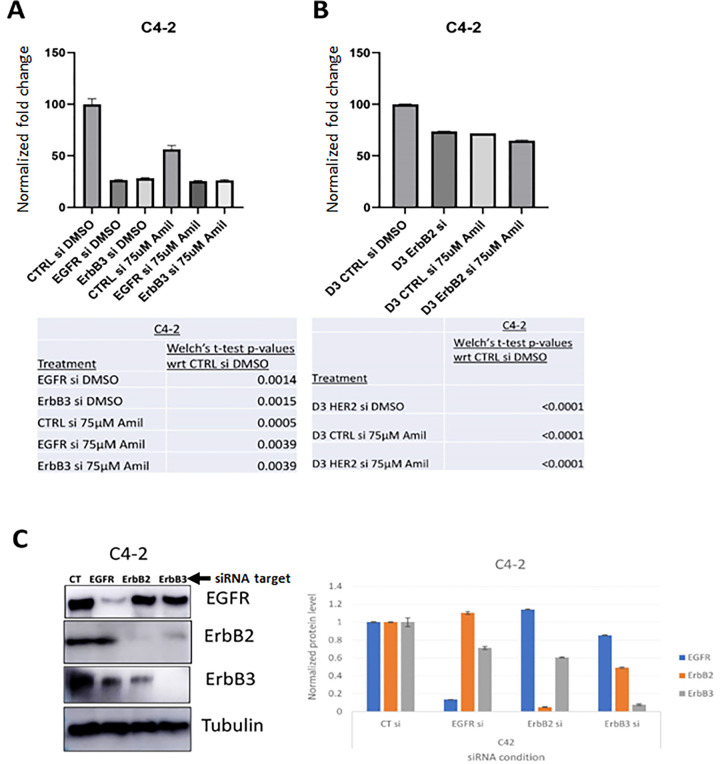
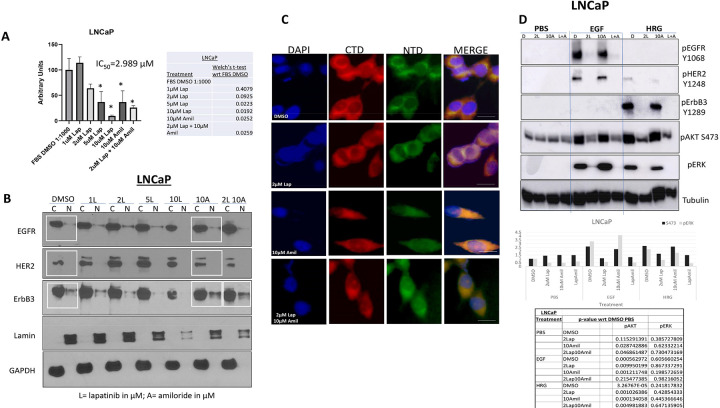
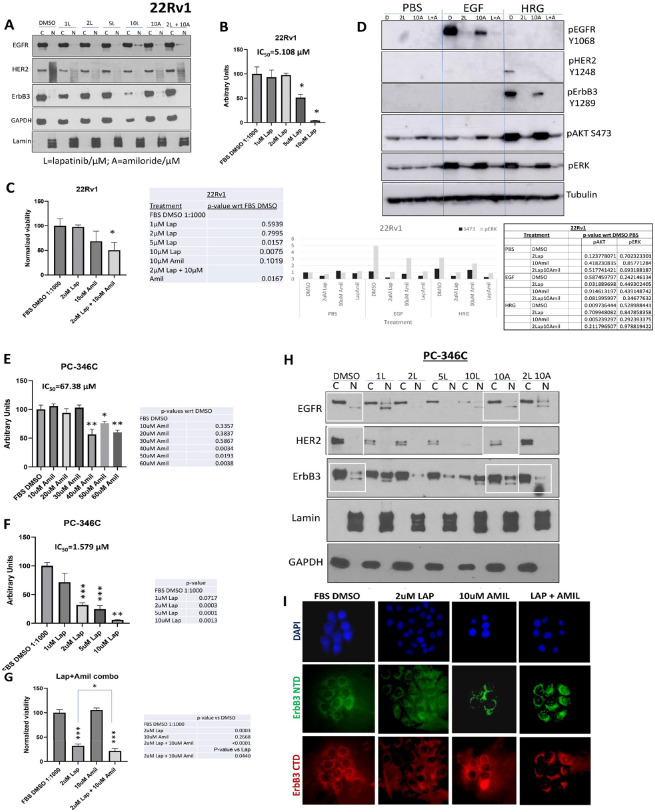
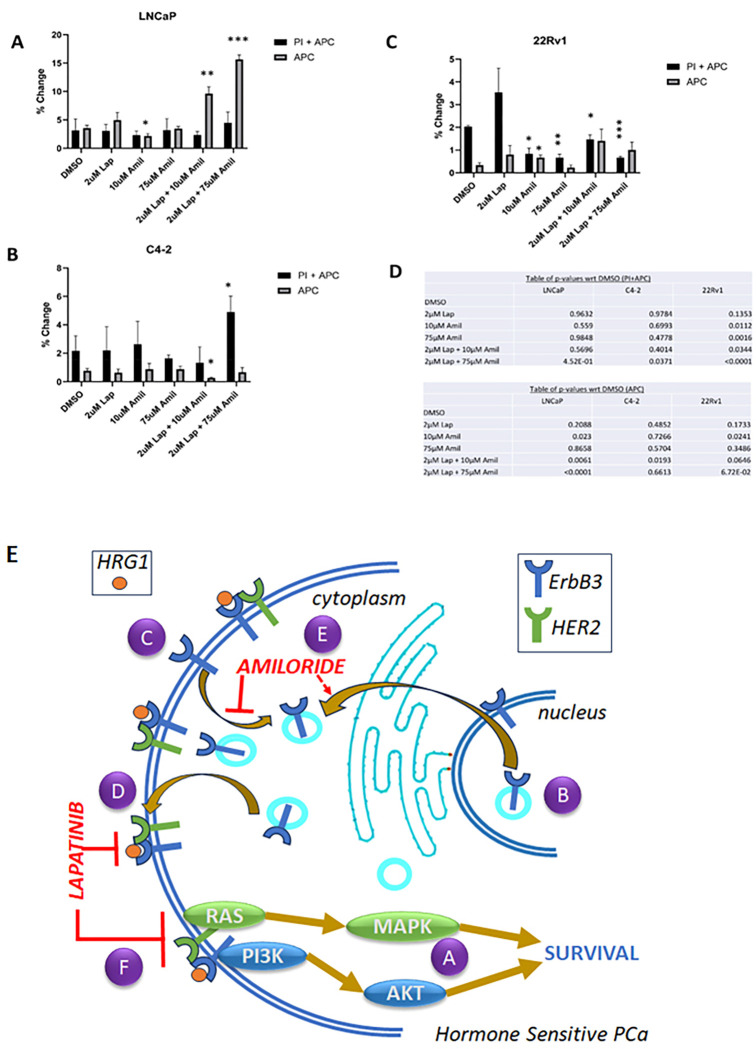
Neoadjuvant therapy (NAT) has been studied in clinically localized prostate cancer (PCa) to improve the outcomes from radical prostatectomy (RP) by 'debulking' of high-risk PCa; however, using androgen deprivation at this point risks castration resistant PCa (CRPC) clonal proliferation with potentially profound side effects such as fatigue, loss of libido, hot flashes, loss of muscle mass, and weight gain. Our goal is to identify alternative NAT that reduce hormone sensitive PCa (HSPC) without affecting androgen receptor (AR) transcriptional activity. PCa is associated with increased expression and activation of the epidermal growth factor receptor (EGFR) family, including HER2 and ErbB3. Dimerization between these receptors is required for activation of downstream targets involved in tumor progression. The FDA-approved HER2 inhibitor lapatinib has been tested in PCa but was ineffective due to continued activation of ErbB3. We now demonstrate that this is due to ErbB3 being localized to the nucleus in HSPC and thus protected from lapatinib which affect membrane localized HER2/ErbB3 dimers. Here, we show that the well-established, well-tolerated diuretic amiloride hydrochloride dose dependently prevented ErbB3 nuclear localization via formation of plasma membrane localized HER2/ErbB3 dimers. This in turn allowed lapatinib inactivation of these dimers via inhibition of its target HER2, which dephosphorylated downstream survival and proliferation regulators AKT and ERK1/2. Amiloride combined with lapatinib significantly increased apoptosis but did not affect AR transcriptional activity. Thus, our data indicate that a combination of amiloride and lapatinib could target HSPC tumors without problems associated with androgen deprivation therapy in localized PCa.
Keywords: Amiloride; ErbB3; androgen receptor; heregulin-1β; lapatinib; prostate cancer; subcellular localization.
Conflict of interest statement
CONFLICTS OF INTEREST: The authors declare that they have no conflicts of interest with the contents of this article.
Figures
References
-
- Eifler JB, Humphreys EB, Agro M, Partin AW, Trock BJ, Han M (2012) Causes of death after radical prostatectomy at a large tertiary center. J Urol 188(3):798–801 - PubMed
-
- Ryan ST, Patel DN, Parsons JK, McKay RR (2020) Neoadjuvant Approaches Prior To Radical Prostatectomy. Cancer J 26(1):2–12 - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
