

Genome-Derived Ampullary Adenocarcinoma Classifier and Postresection Prognostication
- PMID: 39259526
- PMCID: PMC11391358
- DOI: 10.1001/jamasurg.2024.3588
Genome-Derived Ampullary Adenocarcinoma Classifier and Postresection Prognostication
Abstract
Importance: Ampullary adenocarcinoma (AA) is characterized by clinical and genomic heterogeneity. A previously developed genomic classifier defined biologically distinct phenotypes with greater accuracy than standard histologic classification. External validation is needed before routine clinical use.
Objective: To test external validity of the prognostic value of the hidden genome classifier of AA.
Design, setting, and participants: This retrospective cohort study took place at 6 international academic institutions. Consecutive patients (n = 192) who underwent curative-intent resection of histologically confirmed AA were included. The data were analyzed from January 2005 through July 2020.
Exposures: The multilevel meta-feature regression model previously trained on a prospectively sequenced cohort of 3411 patients (1001 pancreatic adenocarcinoma, 165 distal bile duct adenocarcinoma, and 2245 colorectal adenocarcinoma) was applied to AA sequencing data to quantify the relative proportions of parental cell of origin.
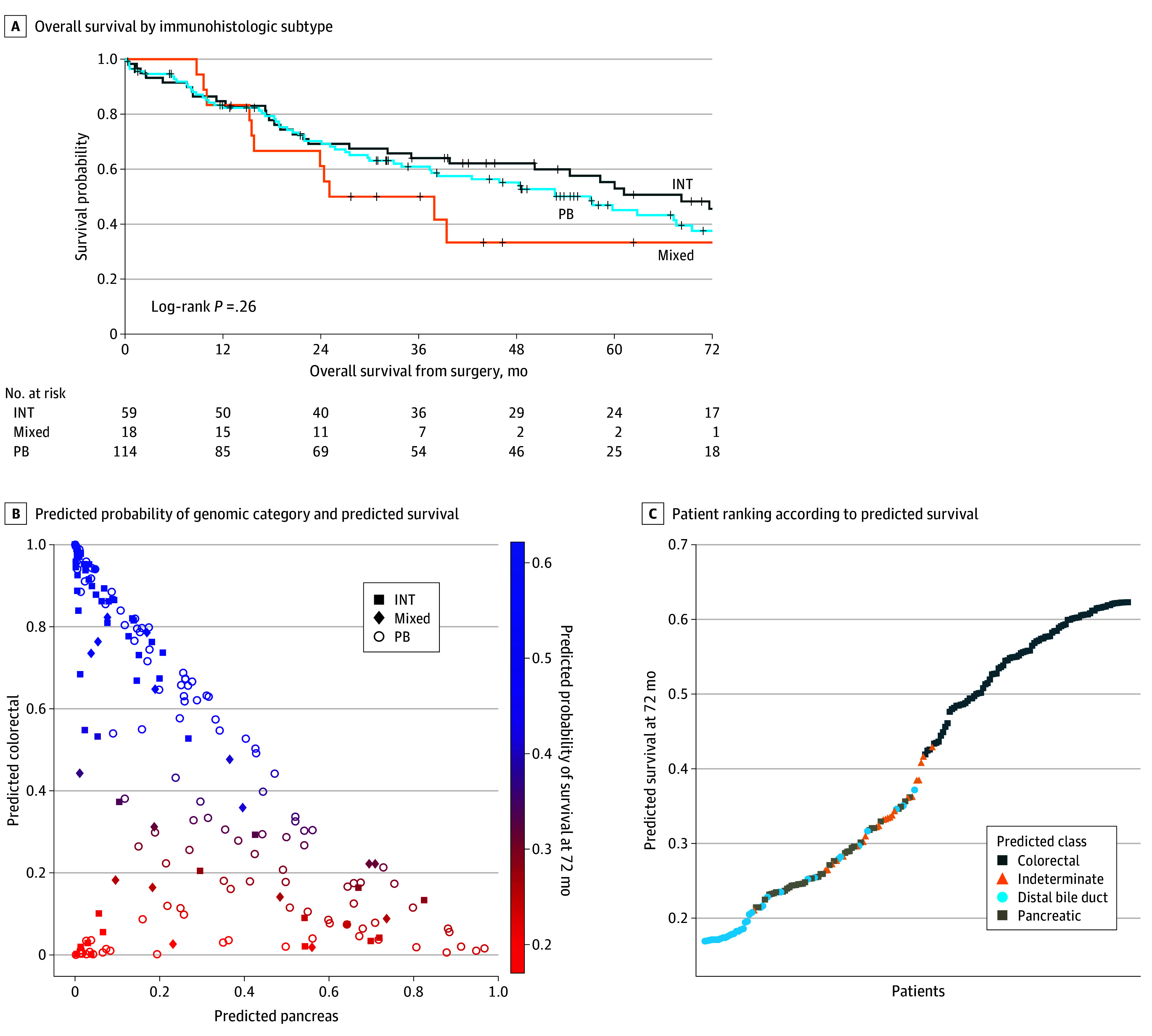
Main outcome and measures: Genomic classification was correlated with immunohistologic subtype (intestinal [INT] or pancreatobiliary [PB]) and with overall survival (OS), using the log-rank test and Cox proportional hazard models.
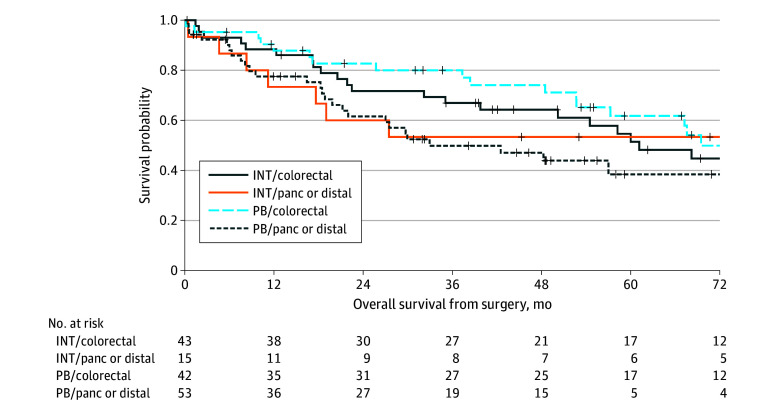
Results: Among 192 patients with AA (median age, 69.0 [IQR, 60.0-74.0] years and 134 were male [64%]), concordance between immunohistologic and genomic subtypes was 55%. Most INT subtype tumors were categorized into the colorectal genomic subtype (43 of 57 [72.9%]). Of the 114 PB subtype tumors, 29 had a pancreatic genomic profile (25.4%) and 24 had a distal bile duct genomic profile (21.1%). Whereas the standard immunohistologic subtypes were not associated with survival (log rank P = .26), predicted genomic probabilities were correlated with survival probability. Genomic scores with higher colorectal probability were associated with higher survival probability; higher pancreatic and distal bile duct probabilities were associated with lower survival probability.
Conclusions and relevance: The AA genomic classifier is reproducible with available molecular testing in a diverse international cohort of patients and improves stratification of the divergent clinical outcomes beyond standard immunohistologic classification. These data provide a molecular classification that may be incorporated into clinical trials for prospective validation.
Conflict of interest statement
Figures

Comment on
-
Ampullary Adenocarcinoma-Advancing Prognostication and Personalized Treatment.JAMA Surg. 2024 Dec 1;159(12):1374. doi: 10.1001/jamasurg.2024.3574. JAMA Surg. 2024. PMID: 39259552 No abstract available.
References
-
- Neoptolemos JP, Moore MJ, Cox TF, et al. ; European Study Group for Pancreatic Cancer . Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: the ESPAC-3 periampullary cancer randomized trial. JAMA. 2012;308(2):147-156. doi: 10.1001/jama.2012.7352 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
