

Randomised controlled trials on radiation dose fractionation in breast cancer: systematic review and meta-analysis with emphasis on side effects and cosmesis
- PMID: 39260879
- PMCID: PMC11388113
- DOI: 10.1136/bmj-2023-079089
Randomised controlled trials on radiation dose fractionation in breast cancer: systematic review and meta-analysis with emphasis on side effects and cosmesis
Abstract
Objective: To provide a comprehensive assessment of various fractionation schemes in radiation therapy for breast cancer, with a focus on side effects, cosmesis, quality of life, risks of recurrence, and survival outcomes.
Design: Systematic review and meta-analysis.
Data sources: Ovid MEDLINE, Embase, and Cochrane Central Register of Controlled Trials (from inception to 23 October 2023).
Study selection: Included studies were randomised controlled trials focusing on conventional fractionation (CF; daily fractions of 1.8-2 Gy, reaching a total dose of 50-50.4 Gy over 5-6 weeks), moderate hypofractionation (MHF; fraction sizes of 2.65-3.3 Gy for 13-16 fractions over 3-5 weeks), and/or ultra-hypofractionation (UHF; schedule of only 5 fractions).
Data extraction: Two independent investigators screened studies and extracted data. Risk of bias and quality of evidence were assessed using the Cochrane Collaboration's tool and the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) approach, respectively.
Data synthesis: Pooled risk ratios (RRs) and hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated using a random effects model. Heterogeneity was analysed using Cochran's Q test and I2 statistic. Network meta-analysis was used to integrate all available evidence.
Main outcome measures: The pre-specified primary outcome was grade ≥2 acute radiation dermatitis and late radiation therapy related side effects; secondary outcomes included cosmesis, quality of life, recurrence, and survival metrics.
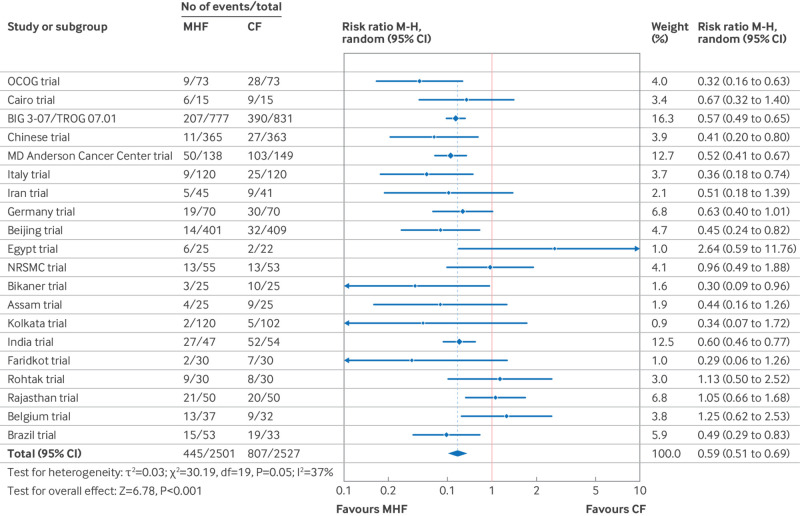
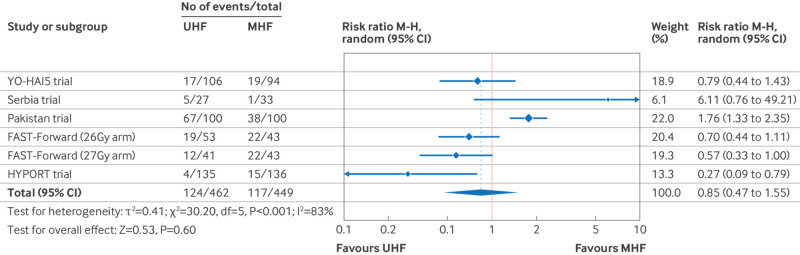
Results: From 1754 studies, 59 articles representing 35 trials (20 237 patients) were assessed; 21.6% of outcomes showed low risk of bias, whereas 78.4% had some concerns or high risk, particularly in outcome measurement (47.4%). The RR for grade ≥2 acute radiation dermatitis for MHF compared with CF was 0.54 (95% CI 0.49 to 0.61; P<0.001) and 0.68 (0.49 to 0.93; P=0.02) following breast conserving therapy and mastectomy, respectively. Hyperpigmentation and grade ≥2 breast shrinkage were less frequent after MHF than after CF, with RRs of 0.77 (0.62 to 0.95; P=0.02) and 0.92 (0.85 to 0.99; P=0.03), respectively, in the combined breast conserving therapy and mastectomy population. However, in the breast conserving therapy only trials, these differences in hyperpigmentation (RR 0.79, 0.60 to 1.03; P=0.08) and breast shrinkage (0.94, 0.83 to 1.07; P=0.35) were not statistically significant. The RR for grade ≥2 acute radiation dermatitis for UHF compared with MHF was 0.85 (0.47 to 1.55; P=0.60) for breast conserving therapy and mastectomy patients combined. MHF was associated with improved cosmesis and quality of life compared with CF, whereas data on UHF were less conclusive. Survival and recurrence outcomes were similar between UHF, MHF, and CF.
Conclusions: MHF shows improved safety profile, cosmesis, and quality of life compared with CF while maintaining equivalent oncological outcomes. Fewer randomised controlled trials have compared UHF with other fractionation schedules, but its safety and oncological effectiveness seem to be similar with short term follow-up. Given the advantages of reduced treatment time, enhanced convenience for patients, and potential cost effectiveness, MHF and UHF should be considered as preferred options over CF in appropriate clinical settings, with further research needed to solidify these findings.
Systematic review registration: PROSPERO CRD42023460249.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work; IC has received consulting fees from Pfizer, Novartis, Eli Lilly, Seagen, Gilead, Astra Zeneca, Daiichi Sankyo, and Menarini StemLine and is a clinical board member of the European Society for Radiotherapy and Oncology (unpaid); JQC has received funding from the Canadian Institutes of Health Research and honorariums from Roche, Pfizer, Novartis, AstraZeneca, Well Doc Alberta, Merck, La Roche-Posay, Knight, Seagen, Oncology Education, and Gilead; no other relationships or activities that could appear to have influenced the submitted work.
Figures
















References
-
- McGale P, Taylor C, Correa C, et al. EBCTCG (Early Breast Cancer Trialists’ Collaborative Group) . Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 2014;383:2127-35. 10.1016/S0140-6736(14)60488-8 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical