

[Multimorbidity as a predictor for inpatient admission in clinical emergency and acute medicine : Single-center cluster analysis]
- PMID: 39261337
- PMCID: PMC12106161
- DOI: 10.1007/s00063-024-01180-6
[Multimorbidity as a predictor for inpatient admission in clinical emergency and acute medicine : Single-center cluster analysis]
Abstract
Background: Parallel to demographic trends, an increase of multimorbid patients in emergency and acute medicine is prominent. To define easily applicable criteria for the necessity of inpatient admission, a hierarchical cluster analysis was performed.
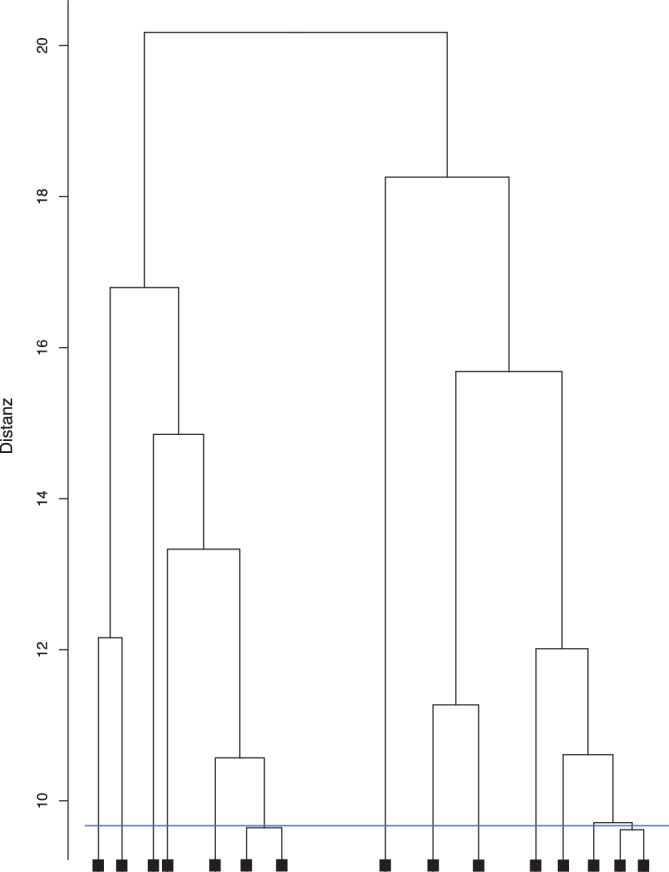
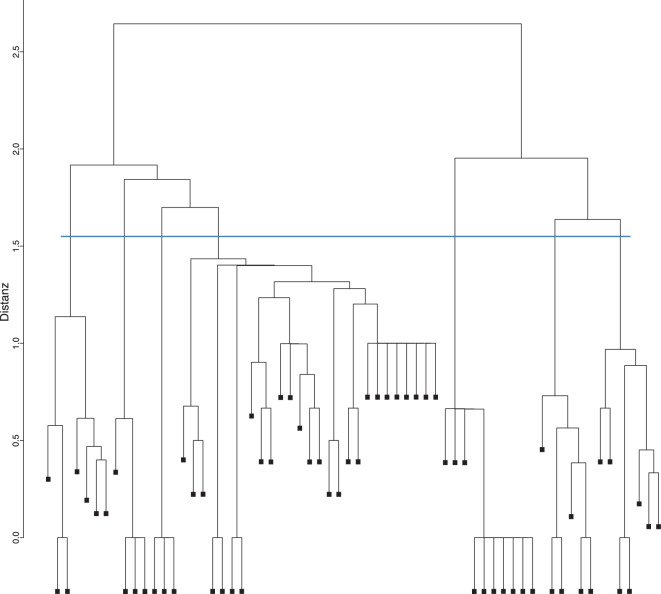
Methods: In a retrospective, single-center study data of n = 35,249 emergency cases (01/2016-05/2018) were statistically analyzed. Multimorbidity (MM) was defined by at least five ICD-10-GM diagnoses resulting from treatment. A hierarchical cluster analysis was performed for those diagnoses initially summarized into 112 diagnosis subclusters to determine specific clusters of in- and outpatient cases.
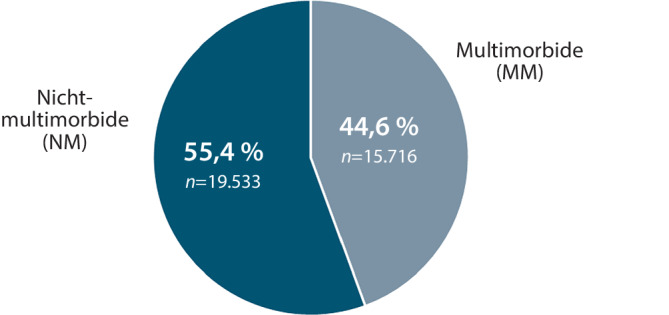
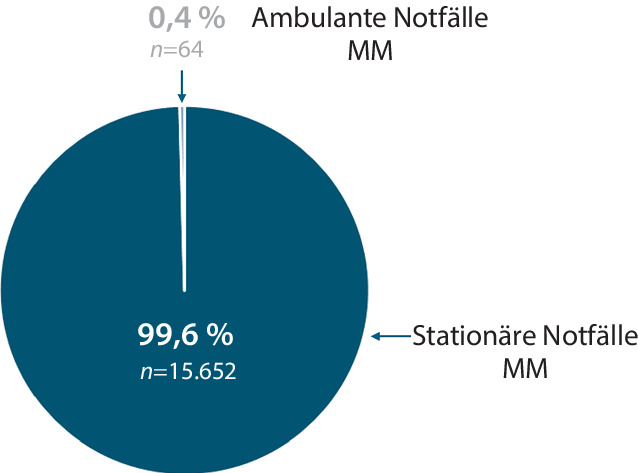
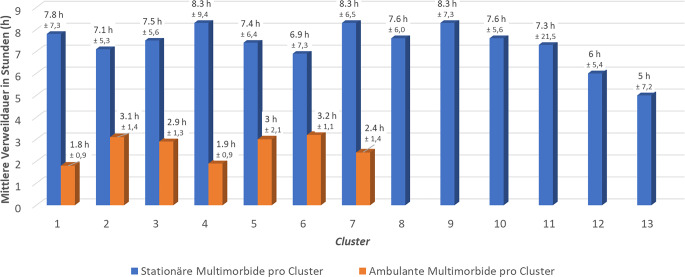
Results: Hospital admission was determined in 81.2% of all ED patients (n = 28,633); 54.7% of inpatients (n = 15,652) and 0.97% of outpatient cases (n = 64) met the criteria for multimorbidity and the age difference between them was highly significant (68.7/60.8 years; p < 0.001). Using a hierarchical cluster analysis, 13 clusters with different diagnoses were identified for inpatient multimorbid patients (MP) and 7 clusters with primarily hematological malignancies for outpatient MP. The length of stay in the ED of inpatient MP was more than twice as long (max. 8.3 h) as for outpatient MP (max. 3.2 h.).
Conclusions: The combination of diagnoses typical for MM were characterized as clusters in this study. In contrast to single or combined single diagnoses, the statistically determined characterization of clusters allows for a significantly more accurate prediction of ED patients' disposition as well as for economic process allocation.
Zusammenfassung: HINTERGRUND: Infolge der demografischen Entwicklung ist ein deutlicher Anstieg von multimorbiden Notfallpatient*innen in der klinischen Notfall- und Akutmedizin in Deutschland zu verzeichnen. Zur Definition operationalisierbarer Kriterien für die Notwendigkeit der stationären Aufnahmeindikation in diesem Patientenkollektiv wurde eine hierarchische Clusteranalyse durchgeführt.
Methodik: In einer retrospektiven, monozentrischen Studie wurden Daten von n = 35.249 Notfällen (01/2016–05/2018) analysiert. Multimorbidität (MM) wurde bei Vorliegen von mehr als 5 im Behandlungsverlauf resultierenden ICD-10-GM-Diagnosen definiert. Es erfolgte eine hierarchische Clusteranalyse der zuvor in 112 Subcluster zusammengefassten Diagnosen zur Ermittlung spezifischer Cluster stationärer und ambulanter Fälle.
Ergebnisse: Stationäre Aufnahmen erfolgten bei 81,2 % aller Notfälle (n = 28.633). Die Kriterien der MM wurden bei 54,7 % der stationären (n = 15.652) und 0,97 % der ambulanten Fälle (n = 64) erfüllt. Der Altersunterschied zwischen letzteren war hochsignifikant (68,7/60,8 Jahre; p < 0,001). Durch hierarchische Clusteranalyse wurden für stationär aufgenommene, multimorbide Patient*innen (MP) 13 Cluster mit unterschiedlichen Diagnosen und für ambulante MP 7 Cluster mit vorrangig hämatologischen Malignomen identifiziert. Die Notaufnahmeverweildauer (VWD) stationärer MP war mehr als doppelt so lang (max. 8,3 h) wie die ambulanter MP (max. 3,2 h).
Schlussfolgerungen: Es wurden für MM typische Diagnosekombinationen in Form von Clustern identifiziert. Im Vergleich zu monodimensionalen oder kombinierten Diagnosen resultiert durch die statistisch erhobene Clusterbildung eine wesentlich genauere Prognose für die Disposition in der klinischen Notfallversorgung als auch für die leistungsrechtliche Prozesszuordnung.
Keywords: Cluster analysis; Disposition; Emergency department; ICD-10-GM diagnose; Multimorbidity.
© 2024. The Author(s).
Conflict of interest statement
Einhaltung ethischer Richtlinien. Interessenkonflikt: E. Grüneberg, R. Fliedner, T. Beißbarth, C.A.F. von Arnim und S. Blaschke geben an, dass kein Interessenkonflikt besteht. Für die Durchführung der Studie liegt ein positives Votum der Ethikkommission der Universitätsmedizin Göttingen vor (Antragsnr. 10/9/21). Für die aufgeführten Studien gelten die jeweils dort angegebenen ethischen Richtlinien.
Figures

References
-
- Gilbert T, Neuburger J, Kraindler J, Keeble E, Smith P, Ariti C, Arora S, Street A, Parker S, Roberts HC et al (2018) Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet 391:1775–1782 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
