

The Efficacy and Safety of Levosimendan in Patients with Advanced Heart Failure: An Updated Meta-Analysis of Randomized Controlled Trials
- PMID: 39261444
- PMCID: PMC11525400
- DOI: 10.1007/s40256-024-00675-z
The Efficacy and Safety of Levosimendan in Patients with Advanced Heart Failure: An Updated Meta-Analysis of Randomized Controlled Trials
Abstract
Background: Intermittent ambulatory levosimendan administration has been shown in several small randomized controlled trials to benefit patients with advanced heart failure, preventing heart failure rehospitalization and mortality. We aim to investigate the totality of high-quality evidence regarding the efficacy and safety of intermittent levosimendan in advanced heart failure patients.
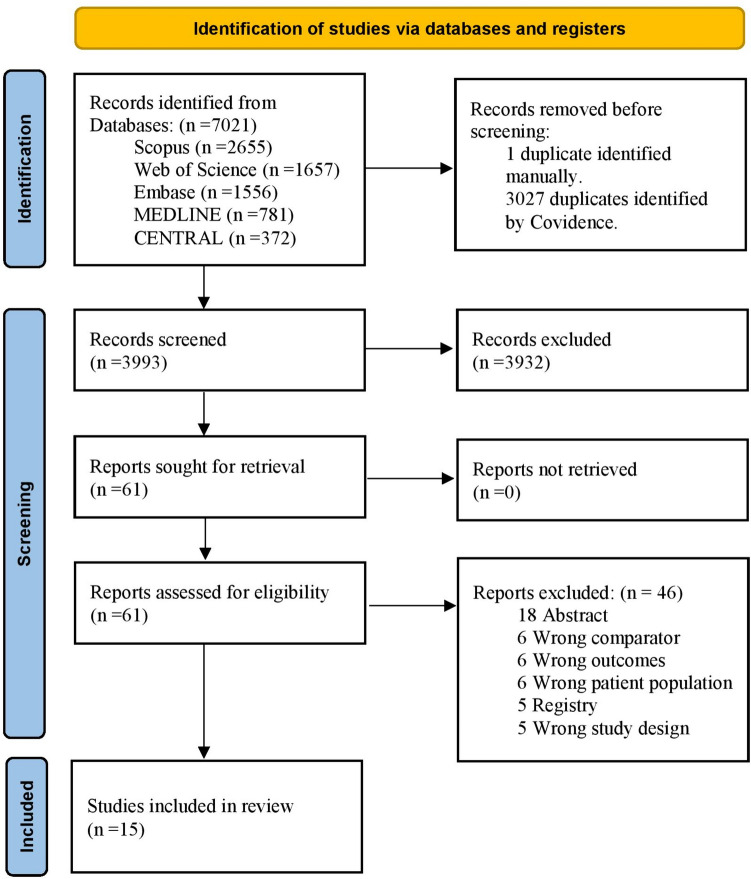
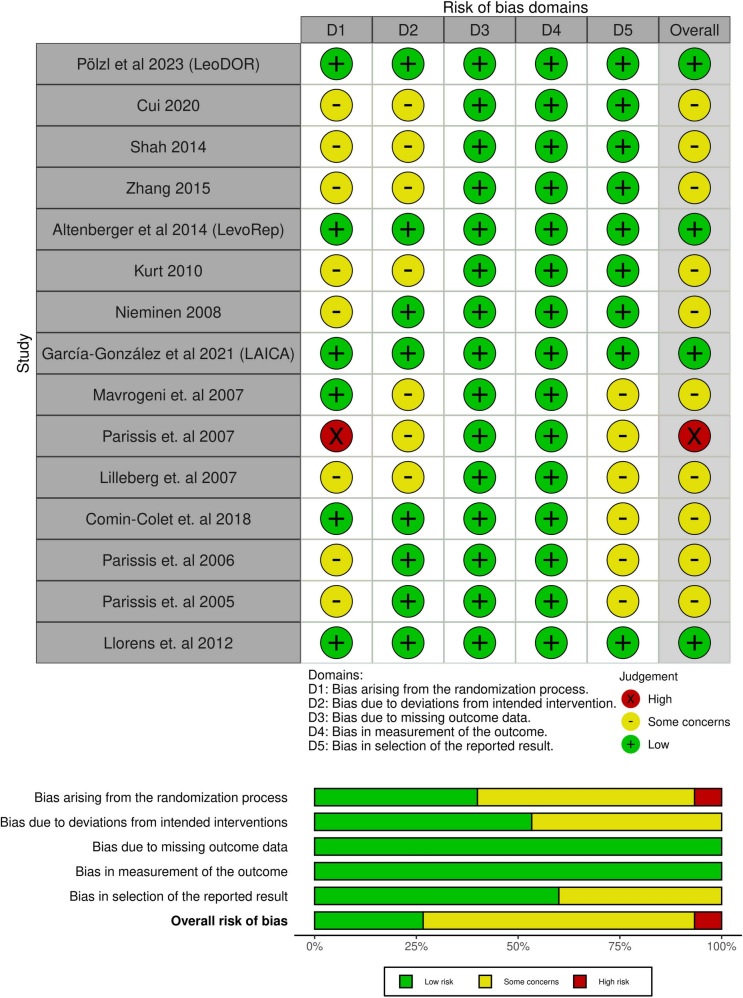
Methods: Up to September 2023, we systematically reviewed the randomized controlled trials indexed in PubMed, Embase Cochrane, SCOPUS, and Web of Science. We used mean difference (MD) to estimate the continuous outcomes, and risk ratio (RR) for the dichotomous outcomes with a 95% confidence interval (CI), using the random-effects model. Ultimately, a trial sequential analysis was employed to enhance the reliability of our findings and Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework for certainty leveling.
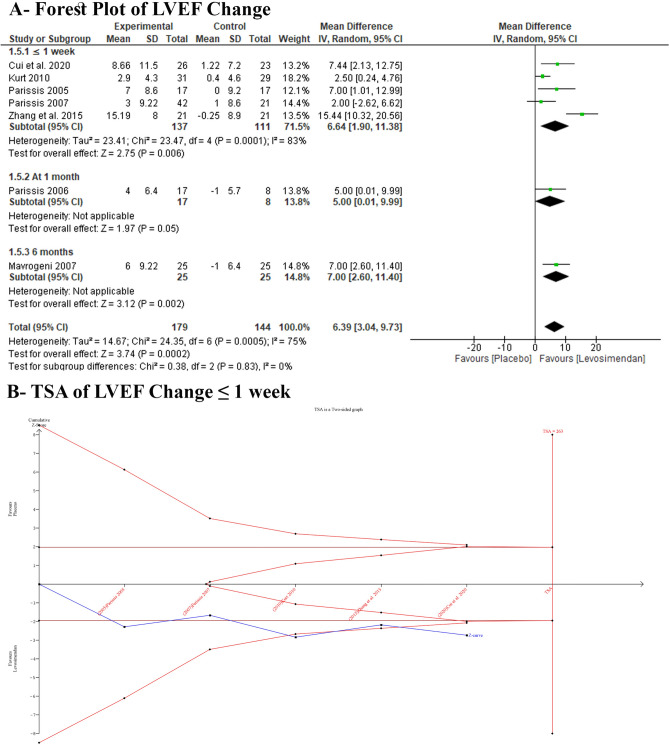
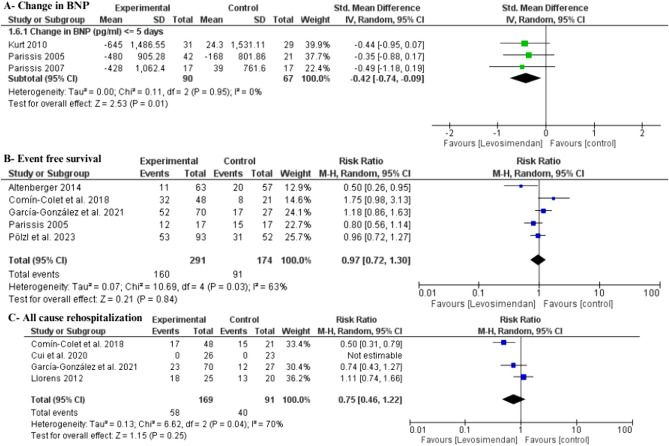
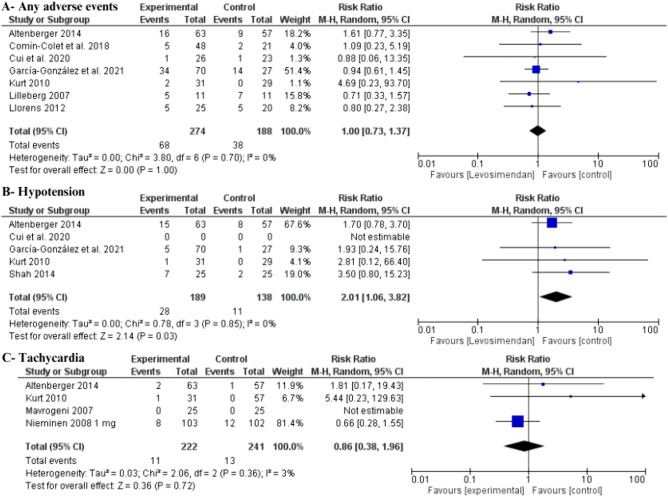
Results: Fifteen randomized controlled trials with 1181 patients were included. Intermittent levosimendan was significantly associated with an improved left ventricular ejection fraction compared with placebo (MD 6.39 [95% CI 3.04-9.73], P = 0.002; I2 = 75, P = 0.0005), with cumulative z-score of change after ≤ 1 week passing the monitoring boundaries, favoring the levosimendan, but did not cross the required information size. Additionally, levosimendan reduced the all-cause mortality rate (RR 0.60 [95% CI 0.40-0.90], P = 0.01; I2 = 9, P = 0.36). However, we found no difference between levosimendan and placebo in all-cause rehospitalization rate (RR 0.75 [95% CI 0.46-1.22], P = 0.25; I2 = 70, P = 0.04), event-free survival rate (RR 0.97 [95% CI 0.72-1.30], P = 0.84; I2 = 63, P = 0.03), or any adverse event (RR 1 [95% CI 0.73-1.37], P = 1.00, I2 = 0%, P = 0.70).
Conclusion: In patients with advanced heart failure, intermittent levosimendan significantly improved left ventricular ejection fraction, brain natriuretic peptide values, and all-cause mortality rate. Levosimendan use is not associated with a change in rehospitalization or event-free survival.
Registration: PROSPERO identifier number (CRD42023487838).
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–858. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
