

Omicron COVID-19 immune correlates analysis of a third dose of mRNA-1273 in the COVE trial
- PMID: 39261482
- PMCID: PMC11390939
- DOI: 10.1038/s41467-024-52348-9
Omicron COVID-19 immune correlates analysis of a third dose of mRNA-1273 in the COVE trial
Abstract
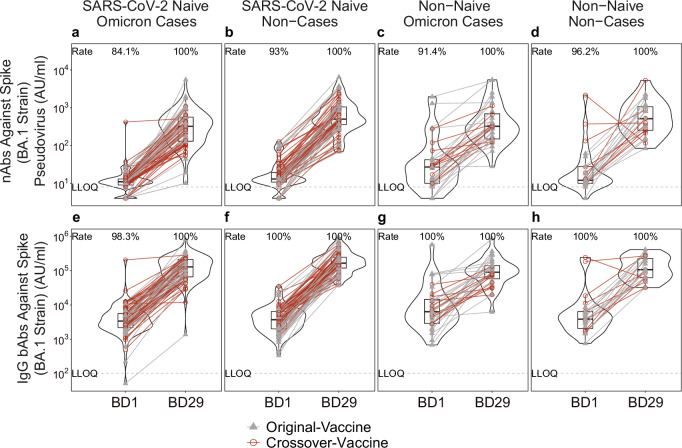
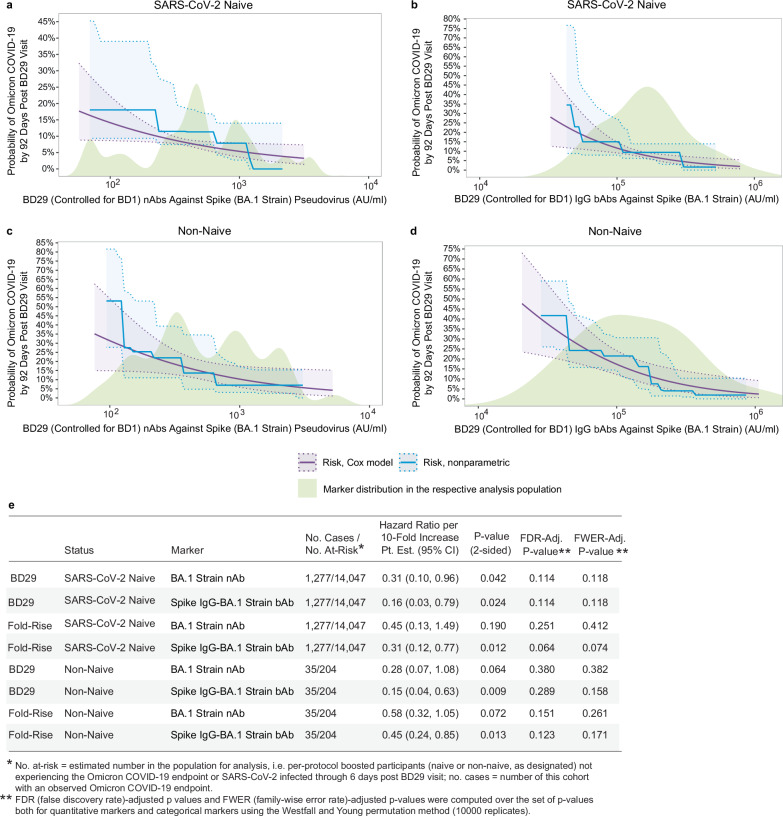
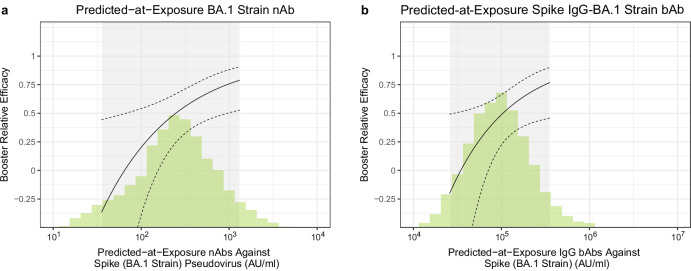
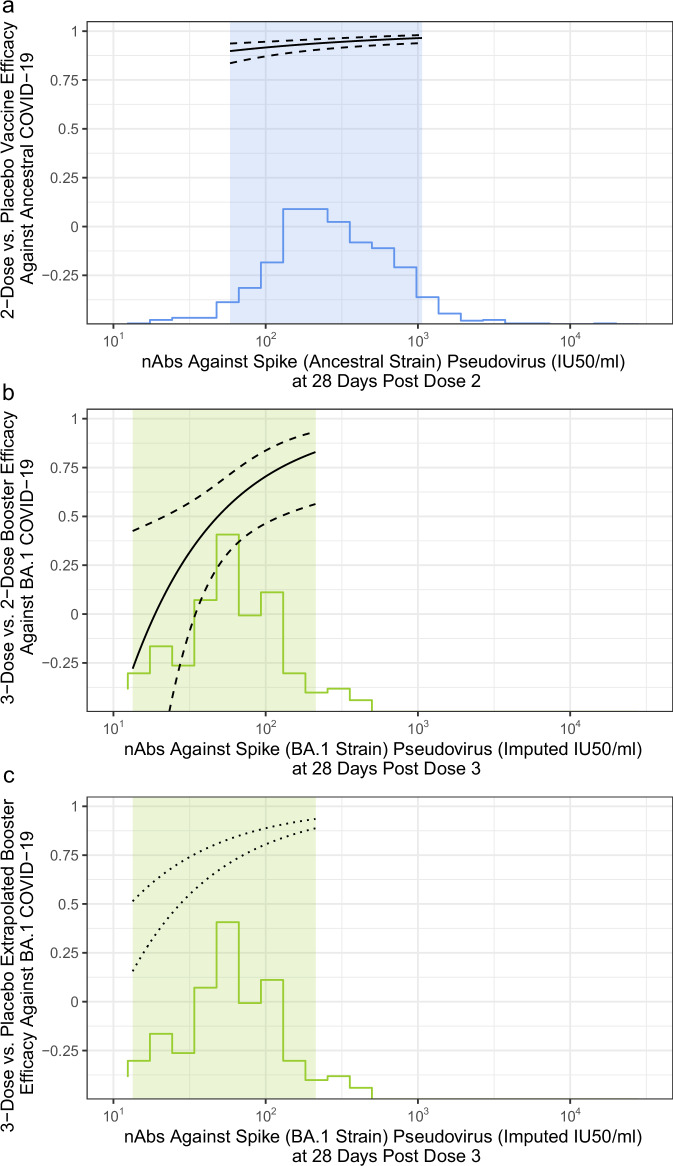
In the phase 3 Coronavirus Efficacy (COVE) trial (NCT04470427), post-dose two Ancestral Spike-specific binding (bAb) and neutralizing (nAb) antibodies were shown to be correlates of risk (CoR) and of protection against Ancestral-lineage COVID-19 in SARS-CoV-2 naive participants. In the SARS-CoV-2 Omicron era, Omicron subvariants with varying degrees of immune escape now dominate, seropositivity rates are high, and booster doses are administered, raising questions on whether and how these developments affect the bAb and nAb correlates. To address these questions, we assess post-boost BA.1 Spike-specific bAbs and nAbs as CoRs and as correlates of booster efficacy in COVE. For naive individuals, bAbs and nAbs inversely correlate with Omicron COVID-19: hazard ratios (HR) per 10-fold marker increase (95% confidence interval) are 0.16 (0.03, 0.79) and 0.31 (0.10, 0.96), respectively. In non-naive individuals the analogous results are similar: 0.15 (0.04, 0.63) and 0.28 (0.07, 1.08). For naive individuals, three vs two-dose booster efficacy correlates with predicted nAb titer at exposure, with estimates -8% (-126%, 48%), 50% (25%, 67%), and 74% (49%, 87%), at 56, 251, and 891 Arbitrary Units/ml. These results support the continued use of antibody as a surrogate endpoint.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
