

Determinants of survival after first relapse of acute lymphoblastic leukemia: a Children's Oncology Group study
- PMID: 39261601
- PMCID: PMC11518984
- DOI: 10.1038/s41375-024-02395-4
Determinants of survival after first relapse of acute lymphoblastic leukemia: a Children's Oncology Group study
Abstract
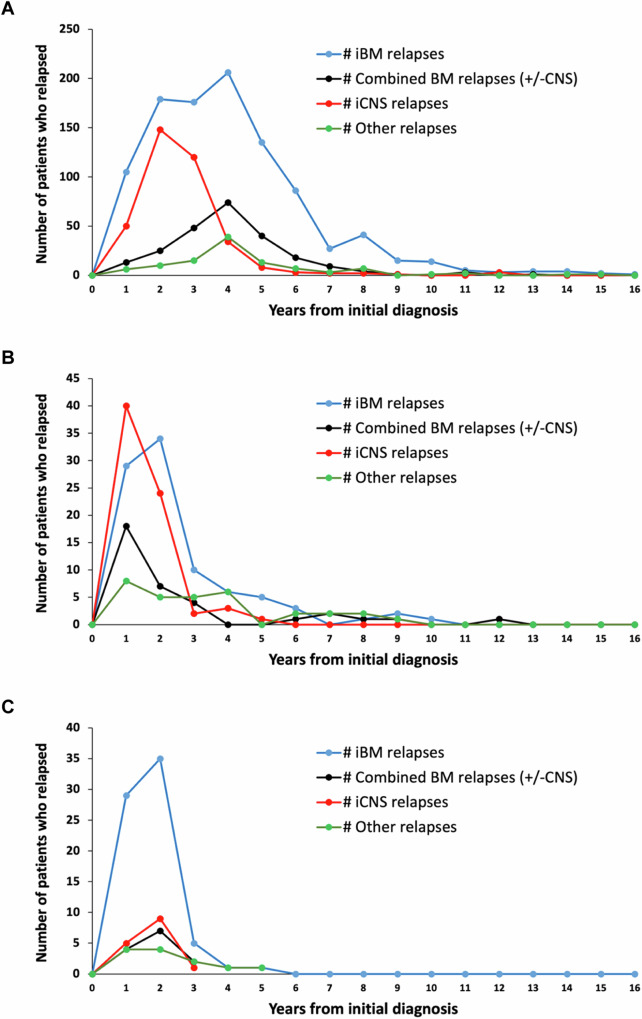
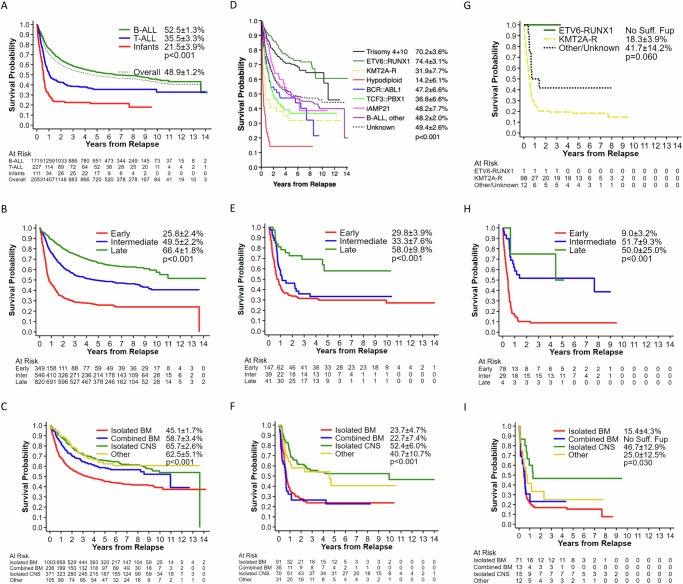
Limited prognostic factors have been associated with overall survival (OS) post-relapse in childhood Acute Lymphoblastic Leukemia (ALL). Patients enrolled on 12 Children's Oncology Group frontline ALL trials (1996-2014) were analyzed to assess for additional prognostic factors associated with OS post-relapse. Among 16,115 patients, 2053 (12.7%) relapsed. Relapse rates were similar for B-ALL (12.5%) and T-ALL (11.2%) while higher for infants (34.2%). Approximately 50% of B-ALL relapses occurred late (≥36 months) and 72.5% involved the marrow. Conversely, 64.8% of T-ALL relapses occurred early (<18 months) and 47.1% involved the central nervous system. The 5-year OS post-relapse for the entire cohort was 48.9 ± 1.2%; B-ALL:52.5 ± 1.3%, T-ALL:35.5 ± 3.3%, and infant ALL:21.5 ± 3.9%. OS varied by early, intermediate and late time-to-relapse; 25.8 ± 2.4%, 49.5 ± 2.2%, and 66.4 ± 1.8% respectively for B-ALL and 29.8 ± 3.9%, 33.3 ± 7.6%, 58 ± 9.8% for T-ALL. Patients with ETV6::RUNX1 or Trisomy 4 + 10 had median time-to-relapse of 43 months and higher OS post-relapse 74.4 ± 3.1% and 70.2 ± 3.6%, respectively. Patients with hypodiploidy, KMT2A-rearrangement, and TCF3::PBX1 had short median time-to-relapse (12.5-18 months) and poor OS post-relapse (14.2 ± 6.1%, 31.9 ± 7.7%, 36.8 ± 6.6%). Site-of-relapse varied by cytogenetic subtype. This large dataset provided the opportunity to identify risk factors for OS post-relapse to inform trial design and highlight populations with dismal outcomes post-relapse.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Vora A, Goulden N, Mitchell C, Hancock J, Hough R, Rowntree C, et al. Augmented post-remission therapy for a minimal residual disease-defined high-risk subgroup of children and young people with clinical standard-risk and intermediate-risk acute lymphoblastic leukaemia (UKALL 2003): a randomised controlled trial. Lancet Oncol. 2014;15:809–18. - DOI - PubMed
MeSH terms
Substances
Grants and funding
- U24 CA114766/CA/NCI NIH HHS/United States
- U10CA13539, U10CA29139/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
- U10CA98543, U10CA98413/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
- U10 CA098543/CA/NCI NIH HHS/United States
- U10CA13539/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
LinkOut - more resources
Full Text Sources
