

Modified tectonic corneoscleral graft technique for treating devastating corneoscleral infections
- PMID: 39261792
- PMCID: PMC11389300
- DOI: 10.1186/s12886-024-03669-2
Modified tectonic corneoscleral graft technique for treating devastating corneoscleral infections
Abstract
Background: This study aims to evaluate the clinical outcomes and efficacy of a modified tectonic corneoscleral graft (TCG) in patients suffering from devastating corneoscleral infections.
Methods: Thirty-eight eyes from 38 patients who underwent the modified TCG were included in this study. The outcomes measured were recurrence rates, best-corrected visual acuity (BCVA), ocular surface stability, postoperative complications, and graft survival.
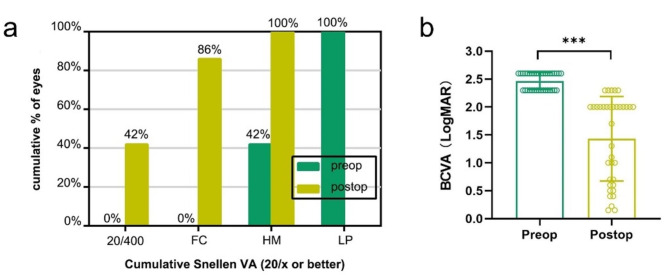
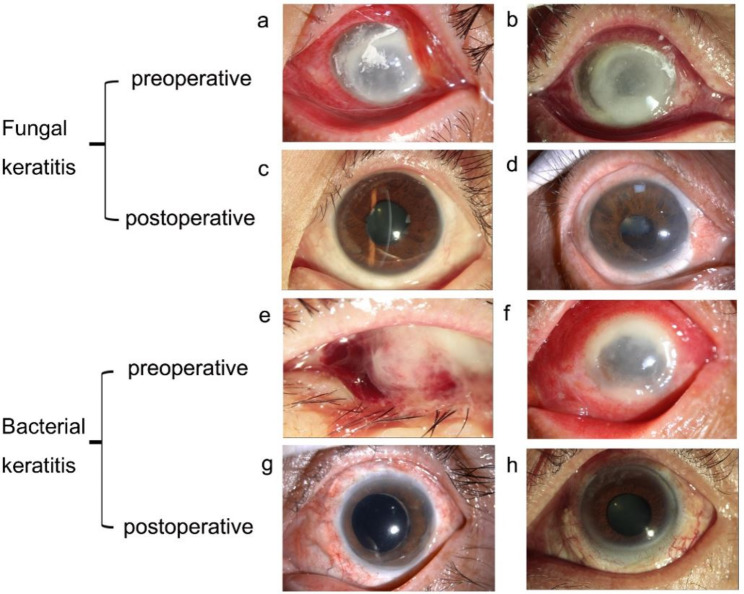
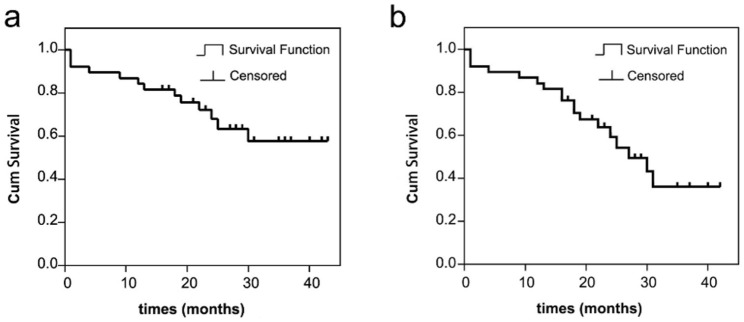
Results: Among the 38 patients, 23 had fungal infections, 9 had bacterial infections and 6 had Pythium insidiosum infections. At the final follow-up, with an average duration of 25.1 ± 8.6 months, the rate of monocular blindness decreased from 100 to 58%. Significant improvements in LogMAR BCVA were observed from preoperative to postoperative measurements (P < 0.001). Thirty-two eyes (84.2%) maintained a stable ocular surface. The survival rate of ocular surface stability was 84.2%±5.9% at one year and 57.7%±9.7% at three years post-surgery. Twenty eyes (52.6%) retained a clear graft, with a survival rate for graft clarity was 81.6%±6.3% at one year and 36.0%±10.8% at three years post-surgery. The incidence of immune rejection was 36.8%. Corneal epithelial defects were observed in ten patients, and choroidal detachment occurred in four patients. No cases of elevated intraocular pressure were detected.
Conclusions: The modified TCG is effective in eradicating infections, preserving the eyeball, and maintaining useful vision in cases of devastating corneoscleral infections. Regular use of tacrolimus, timely administration of glucocorticoids, and good patient compliance can help mitigate postoperative challenges.
Keywords: Corneoscleral graft; Corneoscleral infection; Keratoplasty; Treatment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Large lamellar corneoscleral grafts: tectonic role in initial management of severe ocular chemical injuries.Eur J Ophthalmol. 2016 Jan-Feb;26(1):12-7. doi: 10.5301/ejo.5000631. Epub 2015 Jun 11. Eur J Ophthalmol. 2016. PMID: 26109015
-
Corneoscleral block excision grafts: indications, techniques, and outcomes.Cornea. 2011 Nov;30(11):1277-85. doi: 10.1097/ICO.0b013e3182114124. Cornea. 2011. PMID: 21915049
-
Long-term effect of corneoscleral contact lenses on refractory ocular surface diseases.Cont Lens Anterior Eye. 2019 Aug;42(4):399-405. doi: 10.1016/j.clae.2018.10.011. Epub 2018 Oct 30. Cont Lens Anterior Eye. 2019. PMID: 30389416
-
Infectious interface keratitis (IIK) following lamellar keratoplasty: A literature review.Ocul Surf. 2019 Oct;17(4):635-643. doi: 10.1016/j.jtos.2019.08.001. Epub 2019 Aug 12. Ocul Surf. 2019. PMID: 31415815
-
Vitreoretinal Complications and Outcomes in 92 Eyes Undergoing Surgery for Modified Osteo-Odonto-Keratoprosthesis: A 10-Year Review.Ophthalmology. 2018 Jun;125(6):832-841. doi: 10.1016/j.ophtha.2017.12.003. Epub 2018 Jan 17. Ophthalmology. 2018. PMID: 29342438 Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
