

Early detection and treatment of obstructive sleep apnoea in infants with Down syndrome: a prospective, non-randomised, controlled, interventional study
- PMID: 39262447
- PMCID: PMC11387522
- DOI: 10.1016/j.lanepe.2024.101035
Early detection and treatment of obstructive sleep apnoea in infants with Down syndrome: a prospective, non-randomised, controlled, interventional study
Abstract
Background: Infants with Down syndrome (DS) are at high risk of obstructive sleep apnoea (OSA) which is associated with neurocognitive dysfunction and behaviour problems. The aim of our study was to evaluate the effect of early OSA treatment in infants with DS on neurocognitive development and behaviour.
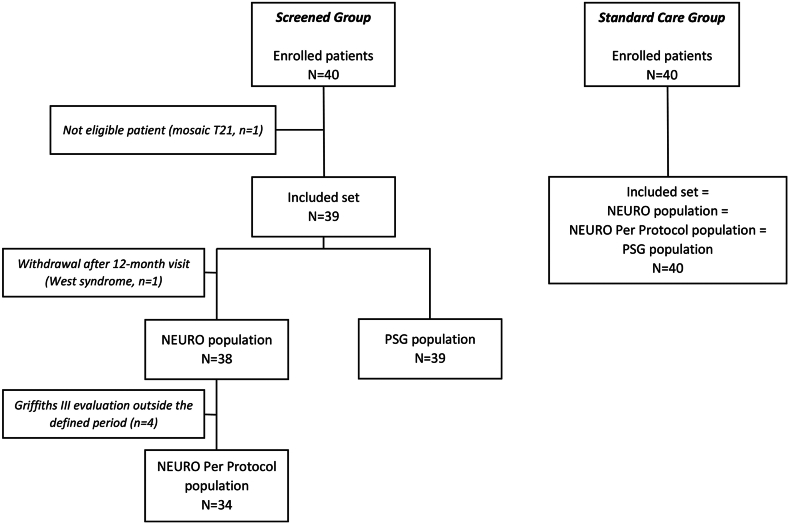
Methods: In this prospective, interventional, non-randomised study, 40 infants with DS underwent polysomnography (PSG) every 6 months in room air between 6 and 36 months of age (Screened Group) and were compared to a control group of 40 infants with DS receiving standard of care and a single, systematic PSG in room air at 36 months of age (Standard Care Group). When present, OSA was treated. The primary endpoint was the total score of the Griffiths Scales of Child Development, Third Edition (Griffiths III) and its subscores at 36 months. Secondary endpoints included a battery of neurocognitive and behaviour questionnaires, and PSG outcomes.
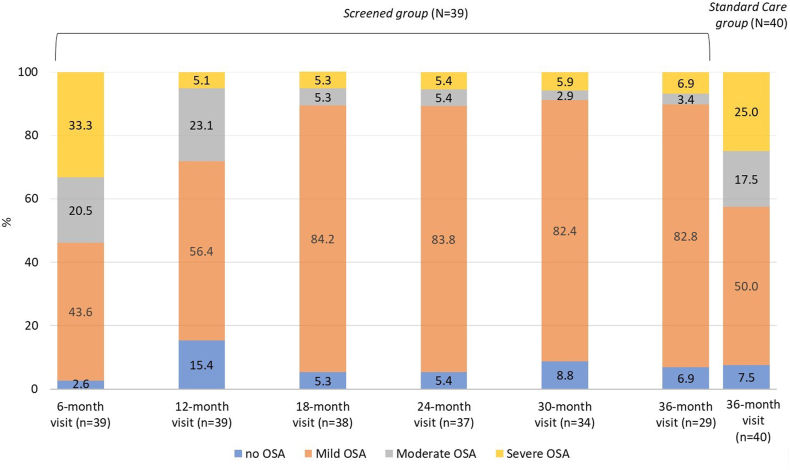
Findings: On the Griffiths III, the total score was significantly higher in the Screened Group compared to the Standard Care Group (difference: 4.1; 95%CI: 1.3; 7.6; p = 0.009). Results in Griffiths III subscores and secondary endpoints were in support of better neurocognitive outcomes in the Screened Group compared with the Standard Care Group. At 36 months, median (Q1; Q3) apnoea-hypopnea index was higher in the Standard Care Group (4.0 [1.5; 9.0] events/hour) compared to the Screened Group (1.0 [1.0; 3.0] events/hour, p = 0.006). Moderate and severe OSA were more frequent in the Standard Care Group as compared to the Screened Group (18.9% versus 3.7% for moderate OSA and 27.0% versus 7.4% for severe OSA).
Interpretation: Early diagnosis and treatment of OSA in infants with DS may contribute to a significantly better neurocognitive outcome and behaviour at the age of 36 months.
Funding: The study was funded by the Jérôme Lejeune Foundation.
Keywords: Behaviour; Down syndrome; Neurocognitive function; Obstructive sleep apnoea; Polysomnography.
© 2024 The Author(s).
Conflict of interest statement
None of the authors had a conflict of interest to declare. A medical writer provided writing and editing assistance, which was funded through the Jérôme Lejeune Foundation.
Figures
References
-
- Parker S.E., Mai C.T., Canfield M.A., et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. 2010;88:1008–1016. - PubMed
-
- Shin M., Besser L.M., Kucik J.E., Lu C., Siffel C., Correa A. Prevalence of Down syndrome among children and adolescents in 10 regions of the United States. Pediatrics. 2009;124:1565–1571. - PubMed
-
- Lafarge C., Larrieu G., Ville I. Why do French women refuse to have Down’s syndrome screening by maternal serum testing? A mixed methods study. Midwifery. 2022;110 - PubMed
-
- Bull M.J. Down syndrome. N Engl J Med. 2020;382:2344–2352. - PubMed
-
- Lal C., White D.R., Joseph J.E., van Bakergem K., LaRosa A. Sleep-disordered breathing in Down syndrome. Chest. 2015;147:570–579. - PubMed
LinkOut - more resources
Full Text Sources
